Form OMB #1123-0NEW OMB #1123-0NEW Application to Restore Federal Firearms Rights
Application to Restore Federal Firearms Rights
OMB #1123-0NEW
Application to Restore Firearms Rights
OMB: 1123-0017
U.S.
Department
of
Justice
0MB
No. 

Office of the Pardon Attorney
Expires: {MM/DD/YYYY)
Application to Restore Federal Firearms Rights

People whose federal firearms rights were lost because of one or more of the below (see 18.U.S.C. §§ 921 & 922(g)):
Felony conviction, i.e., a crime punishable by more than l year in prison
Misdemeanor conviction for a domestic violence offense
Dishonorable discharge from a military branch
A finding of mental incompetency or commitment to a mental treatment facility
Renouncement of U.S. citizenship

Gather all required documents before you submit. Applications that are complete before submission will typically be processed more quickly. The application starts on page 3.
A completed application.
Three character references from persons not related to you by blood or marriage. The character references must have known you for at least 3 years, must be able to attest to certain facts about you, and must explicitly recommend that your federal firearms rights be restored.
Certified court records (if applicable). These could include: indictment or information; plea agreement; factual basis for plea; probation documents prepared in anticipation of sentence; documents of when probation/supervision was terminated; the judgment of conviction; and other relevant court materials.
Mental health records (if applicable). These could include: court or board order for commitment to a mental health facility; petition for commitment; medical and mental health records specifically addressing the diagnosis that allowed the commitment; any order finding restoration of mental competency and rights.
Criminal history of local arrest records (if applicable).
Military conviction, discharge or dismissal paperwork (if applicable). This could include: military service record (DD-214). charge sheet (DD-458); and final PROM order.
Proof of formal renouncement of citizenship (if applicable). This renouncement must have been made before a diplomatic or consular officer of the United States in a foreign state, or before the Attorney General's designee in time of war. See 8 U.S.C. § 1481(a)(S) and (6).
Two fingerprint cards (Standard form FD 258) or equivalent electronic scan.
Authorizations for release of information.
If you have a prior misdemeanor domestic violence conviction, in addition to the certified court records listed above, you should also include:
Official records that include factual information, such as police reports
A record or report disclosing the identity of the victim and relation to applicant if not listed in other documentation.

You may submit no more than 20 attachments per application.
Each attachment can be no more than 30 MB.
The total application submission must be smaller than 600 MB
File Types Allowed with E-Forms applications:
Word (.doc, .docx, docm)
PDF (Portable Document Format)
Excel (.xls, .xlsx, .xlsm)
PowerPoint (.ppt, .pps, .pptx, .pptm)
JPG and JPEG (Joint Photographic Expert Group)
GIF (Graphics and Interchange Format)
File Types Allowed with Paper/Electronic Applications
Fingerprints can be submitted electronically ONLY as an EFT file.
PDF
Where can I find required documents:
Federal Court Documents: PACER (has fees): uscourts.gov/court-records/find-case pacer)
D.C. Cases: dccourts.gov/superior-court/cases-online
Military Records: U.S. Department of Veteran's Affairs: va.gov/records/get-military service-records/
State Documents: Contact local jurisdiction
Application to Restore Federal Firearms Rights

Answer questions as accurately and as fully as you can, to the best of your knowledge.
Making any intentionally false statements of material facts may be a reason for denying your application. In addition, the knowing and willful falsification of a document submitted to the government may subject you to criminal punishment, including up to five years' imprisonment and a $250,000 fine. See 78 U.S.C. §§ 7007 and 3577.
Section 1

Full name {Last, First, Middle) |
Date of birth {MM/DD/YYYY) |
SSN (999-99-9999) |
If different, full name at time of conviction (i.e. married, maiden or aliases)
Full
name
(Last,
First,
Middle)
Place of birth
Country |
State |
City |
Country of citizenship
 United
States
of
America
(U.S.A.)
United
States
of
America
(U.S.A.)

Yes No
Demographics
Sex (M/F)
Male Female
Race (Check all that apply)
Alaska Native or American Indian Asian
Hispanic or Latino (Yes/No)
Yes No
Black or African American White
Native Hawaiian/Pacific Islander Other
Federal firearm license (if applicable) FBI number (if applicable)

Physical address and contact information
-
Street Address
Unit number
City
State
Zip code
Email
Phone (999-999-9999)
Mailing address (if different from physical address)
Street address |
Unit number |

City State |
Zip code |
Email is the best way to contact you. If you do not have an email, you can share the email of a trusted person, or a phone number. If an attorney is helping you with this application, share their contact information.
Attorney information



You must provide a local arrest record for every place where you have lived in the last 25 years, or since the age of 18, whichever is longer. You must provide an arrest record for every entry, even if you have not been arrested in that locality. Include the city, state, and approximate amount of time you have lived there. If you were arrested in a place that you did not live, you can provide that information in section C. Any additional localities must be listed in the "additional locality" attachment at the end of the application.
I am attaching an arrest record in this locality Yes No

I am attaching an arrest record in this locality Yes No

I am attaching an arrest record in this locality Yes No


Provide an arrest record from any locality where you have been arrested, but may not have lived. The arrest record can be a certificate from local law enforcement agency that details the charges, dates, and outcomes of each arrest. If you have already included a record in section B, you do not need to include again here. If you need additional space, use the "additional local arrests" attachment at the end of the application.
-
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
I have attached all local arrest records
Section 2

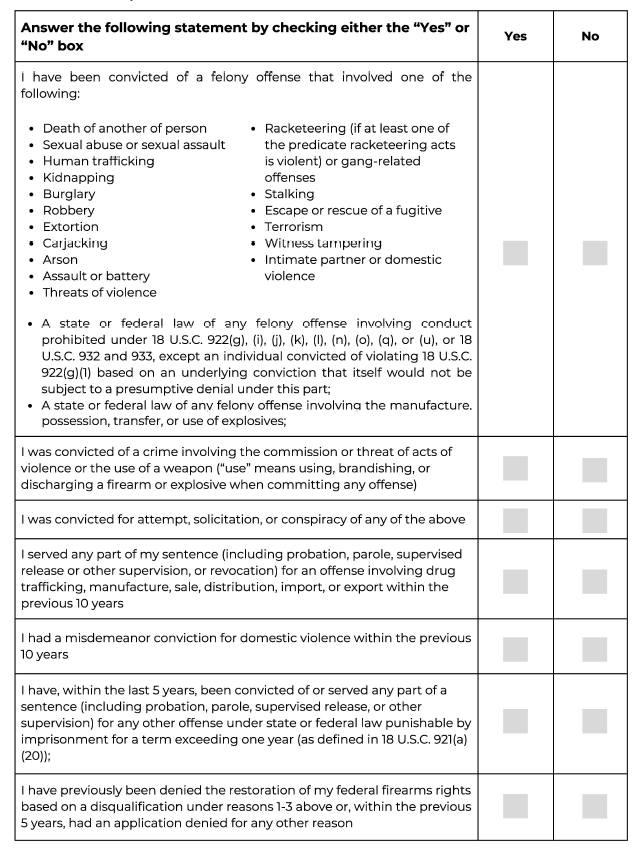
Answer each question below:


Section 3

Federal felony conviction Yes No

You
must
report all
convictions
for
separate
counts.
For
multiple
counts
under
the same
statute,
you
only
need
to
list
the
statute
once.
List
all
additional
convictions
using
"additional
convictions"
attachment at the end of the application.
You must attach a certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.

Other supporting documents I am submitting
Check all that apply. (You must include at least one document that contains factual information about the offense.)
Judgment
Indictment or information
Presentence report Other Plea agreement and/or factual basis
State felony conviction Yes No
You must report all convictions for separate counts. For multiple counts under the same statute, you only need to list the statute once. List all additional convictions using "additional convictions" attachment at the end of the application.
You must attach a certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.

Other supporting documents I am submitting
Check all that apply. (You must include at least one document that contains factual information about the offense.)
Judgment
Indictment or information
Presentence report Other Plea agreement and/or factual basis
Misdemeanor domestic violence conviction Yes No
You must report all convictions. You must attach all local arrest records. If you have more than one conviction, list all additional convictions using "additional convictions" attachment at the end of the application.
You must attach:
l. A certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.
2. A record, report, or document that discloses the victim's identity and relationship to you

Other supporting documents I am submitting
Check all that apply. (You must include at least one document that contains factual information about the offense.)
Judgment
Indictment or information
Presentence Report Other Plea Agreement and/or Factual Basis
Police Report or other factual information about the offense
Dismissal or dishonorable discharge from a military branch Yes No
Date
of
discharge
(MM/DD/YYYY)
Army
Marine Corps
Navy
Coast Guard
Air Force Space Force
Military branch conviction Yes No
You must report all convictions for separate counts. For multiple counts under the same statute, you only need to list the statute once. List all additional convictions using "additional convictions" attachment at the end of the application.

You must attach a certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.

Other supporting documents I am submitting
Check all that apply. (You must include at least one document.)
DD-214 DD-258 Other
PROM order Report of the result of trial (RRoT)/Statement of trial results (STR) or equivalent court-martial record
A finding of mental incompetency or commitment to a mental treatment facility Yes No

You
must
report
all
findings
of
incompetency
or
commitments.
For
more
than
one
finding
or
commitment,
list
additional
commitments
on
"additional
information"
attachment
at
the
end
of
the application.
Other supporting documents I am submitting
Check all that apply. (You must include at least order of restoration)
Court or board order for commitment to mental health facility Order finding restoration of mental competency and rights
Medical health records
Petition for commitment Other
Renouncement of U.S. citizenship
Yes No

Other supporting documents I am submitting
Check all that apply.
Consular document acknowledging renouncement Other
Section 4

List three references. References must be people not related to you by blood or marriage, who have known you for at least three years, and who are willing to make all affirmations included on the Character Reference Sheet.
Character Reference 1
-
Full name (Last, First, Middle)
Street Address
Unit number
City
State
Zip code
Email
Phone (999-999-9999)
On behalf of _ I, certify that (check all that apply):
Name of applicant
I have known the applicant for over 3 years
I am not related to the applicant by blood or marriage
I have never been convicted in any court of a crime punishable by a term of imprisonment exceeding one year
I further certify that to my knowledge, the applicant:
Has not committed any crime, other than traffic or other minor infractions, within the past five years
Is not a regular user of illegal drugs
Does not regularly abuse alcohol or other intoxicants
Is not currently suffering from a mental health condition that would impair the applicant’s judgment or behavior
Is a person of good character and has a good reputation in the community
Have not used violence or threatened to use violence against an person even if authorities were not notified
Would not pose a danger to public safety if permitted to possess a firearm
I recommend that the applicant's federal firearms rights be restored.
Under penalty of perjury, I certify that the above information is true and correct to the best of my knowledge, information, and belief.

Character Reference 2
-
Full name (Last, First, Middle)
Street Address
Unit number
City
State
Zip code
Email
Phone (999-999-9999)
On behalf of _ I, certify that (check all that apply):
Name of applicant
I have known the applicant for over 3 years
I am not related to the applicant by blood or marriage
I have never been convicted in any court of a crime punishable by a term of imprisonment exceeding one year
I further certify that to my knowledge, the applicant:
Has not committed any crime, other than traffic or other minor infractions, within the past five years
Is not a regular user of illegal drugs
Does not regularly abuse alcohol or other intoxicants
Is not currently suffering from a mental health condition that would impair the applicant's judgment or behavior
Is a person of good character and has a good reputation in the community
Have not used violence or threatened to use violence against an person even if authorities were not notified
Would not pose a danger to public safety if permitted to possess a firearm
I recommend that the applicant's federal firearms rights be restored.
Under penalty of perjury, I certify that the above information is true and correct to the best of my knowledge, information, and belief.

Character Reference 3
-
Full name (Last, First, Middle)
Street Address
Unit number
City
State
Zip code
Email
Phone (999-999-9999)
On behalf of _ I, certify that (check all that apply):
Name of applicant
I have known the applicant for over 3 years
I am not related to the applicant by blood or marriage
I have never been convicted in any court of a crime punishable by a term of imprisonment exceeding one year
I further certify that to my knowledge, the applicant:
Has not committed any crime, other than traffic or other minor infractions, within the past five years
Is not a regular user of illegal drugs
Does not regularly abuse alcohol or other intoxicants
Is not currently suffering from a mental health condition that would impair the applicant's judgment or behavior
Is a person of good character and has a good reputation in the community
Have not used violence or threatened to use violence against an person even if authorities were not notified
Would not pose a danger to public safety if permitted to possess a firearm
I recommend that the applicant's federal firearms rights be restored.
Under penalty of perjury, I certify that the above information is true and correct to the best of my knowledge, information, and belief.

How will this information be used under the Privacy Act:
The purpose for collecting this information is to determine your eligibility for relief under 78
U.S.C. § 925(c) and 28 C.F.R. § 107.1 to determine whether restoration of federal firearms rights should be issued. The routine uses of this information include making determinations on eligibility. Information will also be disclosed to other Federal, State, foreign, and local law enforcement and regulatory agencies to verify information provided on the application. [TBD]. You must provide the requested information to apply for a restoration of your rights. Failure to do so will result in a denial and an inability to process the application. Solicitation of your social security number is made pursuant to 78 U.S.C. § 925(c), and E.O. 9397, and it will be used to verify your identity. If granted, your name, address, court of conviction, and date of conviction will be published in the Federal Register, as required by 78 U.S.C. § 925(c). You must consent to this disclosure in order to apply for restoration of your federal firearms rights.

Paperwork Reduction Act Notice
This collection meets the requirements of 44 U.S.C. § 3507, as amended by the Paperwork Reduction Act of 7995. We estimate that it will take 60 minutes to read the instructions, gather the relevant materials, and answer questions on the form. Send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to Attn: Office of the Pardon Attorney, U.S. Department of Justice, Attn: 0MB Number xxxx-xxxx, RFK Building, 950 Pennsylvania Avenue, N.W., Washington, D.C. 20530. The 0MB clearance number, xxxx-xxxx, is currently valid. PARDON may not collect this information, and you are not required to respond, unless this number is displayed.
How long will it take to get a decision
We strongly encourage applicants to use the online application at www.justice.gov/FFRR to ensure the fastest processing times. Paper applications will take significantly longer to process. Once received, the process will follow the below steps, and it may take a lengthy period of time for a decision to be issued.

Carefully read this authorization, and if you agree, sign and date in ink.
I authorize any investigator, special agent, or other duly accredited representative of the Department of Justice, the Department of Defense, and any other authorized Federal agency, to obtain any information relating to my activities from schools, residential management agents, employers, criminal justice agencies, retail business establishments, courts, or other sources of information. This information may include, but is not limited to, my academic, residential, achievement, performance, attendance, disciplinary, employment history, criminal history, arrest, conviction, including the presentence investigation report, if any, medical, psychiatric/psychological, health care, and financial and credit information.
I further authorize the Department of Justice, the Department of Defense, and any other authorized Federal agency, to request criminal record information about me from criminal justice agencies for the purpose of determining my suitability for relief from disabilities under 18 U.S.C. § 925(c) and 28 C.F.R. § 107.1.
I authorize custodians of records and sources of information pertaining to me to release such information upon request of the investigator, special agent, or other duly accredited representative of any Federal agency authorized above regardless of any previous agreement to the contrary. I understand that the information released by records custodians and sources of information is for official use by the Federal Government only for the purposes of processing my application for relief from disabilities under 18 U.S.C. § 925(c) and 28 C.F.R. § 107.1, and may be redisclosed by the Government only as authorized by law.
Copies of this authorization that show my signature are as valid as the original release signed by me. If not previously revoked in writing, this Authorization is valid and shall remain in effect so long as I am under consideration for relief from disabilities under l8
U.S.C. § 925(c) and 28 C.F.R. § 107.1.
Signature |
Date (MM/DD/YYYY) |
|
Full name (Last, First, Middle) |
DOB (MM/DD/YYYY) |
SSN (999-99-9999) |
Street Address |
Unit number |
|
City |
State |
Zip code |
Phone (999-999-9999) |
||

Carefully read this authorization, and if you agree, sign and date in ink.
This is a release for the Department of Justice, any authorized representative of the Department of Justice, and any investigator, special agent, or other duly accredited representative of the Federal Bureau of Investigation to obtain from your mental health care practitioner(s) information relating to the mental health counseling/psychotherapy you have disclosed in connection with your application for relief from disabilities under 78
U.S.C. § 925{c) and 28 C.F.R § 107.1. Your signature below will allow the practitioner(s) to provide such information upon the request of any of the individuals listed above.
I am seeking relief from disabilities under 78 U.S.C. § 925(c) and 28 C.F.R § 107.1 and to facilitate the processing of my application for relief from disabilities, I hereby authorize the Department of Justice, any authorized representative of the Department of Justice, and any investigator, special agent, or other duly accredited representative of the Federal Bureau of Investigation to obtain from my mental health care practitioner(s) information concerning any diagnosis, prognosis, treatment or referral for treatment relating to, or arising out of, my participation in mental health counseling/psychotherapy from
to the present, including, without limiting the scope of the information, the nature, extent and duration of the condition(s) for which mental health counseling/psychotherapy was received, the effects of the condition(s), past or current treatment for the condition(s), and any prognosis for each.
I understand the information released pursuant to this Authorization for Release is for official use by the Federal Government for the purposes provided in connection with the processing of my application for relief from disabilities under 78 U.S.C. § 925{c) and 27 C.F.R.
§ 478.744, which may include redisclosure of the information to persons concerned with the process, and may be otherwise redisclosed by the Government only as authorized by law.
Copies of this Authorization that show my signature are as valid as the original Authorization signed by me. This Authorization is subject to revocation at any time except to the extent that the practitioner who is to make the disclosure or any person who is authorized to receive the information hasalready taken action in reliance on it. If not previously revoked in writing, this Authorization is valid and shall remain in effect so long as I am under consideration for relief from disabilities under 78 U.S.C. § 925{c) and 28 C.F.R § 107.1.
Signature |
Date (MM/DD/YYYY) |
|
Full name (Last, First, Middle) |
DOB (MM/DD/YYYY) |
SSN (999-99-9999) |
Street Address |
Unit number |
|
City |
State |
Zip code |
Phone (999-999-9999) |
||

Additional conviction Federal felony State felony Misdemeanor domestic violence You must report all convictions for separate counts. For multiple counts under the same statute, you only need to list the statute once.

You must attach a certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.

Other supporting documents I am submitting
Check all that apply. (You must include at least one document that contains factual information about the offense)
Judgment
Indictment or information
Additional conviction
Presentence report Other Plea agreement and/or factual basis
Federal felony State felony Misdemeanor domestic violence
You must report all convictions for separate counts. For multiple counts under the same statute, you only need to list the statute once.

You must attach a certified document from a relevant authority, citing the date of completion of your sentence, including any term of supervision.

Other supporting documents I am submitting
Check all that apply. (You must include at least one document that contains factual information about the offense)
Judgment
Indictment or information
Presentence report Other Plea agreement and/or factual basis

I am attaching an arrest record in this locality Yes No

I am attaching an arrest record in this locality Yes No

I am attaching an arrest record in this locality Yes No

I am attaching an arrest record in this locality Yes No



-
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State
Arrest month/year (MM/YYYY)
City
State

{Chief Law Enforcement Officer Name (Last, First)}
{Title}
{Locality}
{Email}
{Date}
I am currently under a federal disability that prevents me from possessing a firearm under federal law, 78 U.S.C. 922(g). This document serves as notice that I am applying to the United States Attorney General to restore my federal firearm rights under 78 USC 925c & 28 CFR 107.1. Though you are not required to do so, if you would like to either support or oppose the application, you may do so by (mechanism for submitting comments) within 14 days of the date of this notice. Include my full name [FULL NAME here] in the subject line of any correspondence.
The Department will provide you notice of the final decision. Also, note that if granted this relief, I will be allowed to posses a firearm under federal law, but this relief does not necessarily free me from any state disabilities that may remain.
{Signature}
{Full name (Last, First, Middle)}
{Street address}
{City, State Zip code}
{Email address}
{Phone number (999-999-9999)}
Page

| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Copy of Beige and Brown Simple Bordered Job Application Form (5).pdf |
| Author | Ogbe, Abiel M. |
| File Modified | 0000-00-00 |
| File Created | 2025-08-03 |
© 2026 OMB.report | Privacy Policy