Survey
A Study of Feedback in Teacher Evaluation Systems
KAttach B Copy of Survey & Online Survey Screen Shots
A Study of Feedback in Teacher Evaluation Systems
OMB: 1850-0903
Attachment B: Survey of Rural SIG School Principals
This confidential survey is part of a study of the implementation of School Improvement Grants (SIG) in rural schools using the transformation model. The Regional Educational Laboratory (REL) Northwest is conducting this study. REL Northwest is a private nonprofit research and technical assistance provider based in Portland, Oregon, that is part of the Institute of Education Sciences’ Regional Educational Laboratory program (http://ies.ed.gov/ncee/edlabs/).
The purpose of this study is to provide educators and policymakers with information about how rural schools implemented their SIG and to inform future efforts to turn around schools in rural areas. Your responses are very important because, as the principal of a SIG school, you have first-hand knowledge about your school’s implementation efforts. We will combine your answers with those of other SIG principals to help evaluators understand the implementation of the SIG transformation model in rural schools.
The survey takes about 20 minutes to complete. We request that you respond by [date to come].
Responses to this survey are completely confidential. Because your participation is voluntary, there are no repercussions to participating or not participating. By completing this survey you are consenting to the inclusion of your survey data in the REL study. No one, other than the researchers working on this project from REL Northwest and Policy Studies Associates, will see your individual responses, and personal information will be removed from the database before analysis. Furthermore, the reports prepared for this study will summarize findings across the sample and will not associate responses with a specific district, school, or individual. Any reported information will always be aggregated across multiple schools. We will not provide information that identifies you or your district to anyone outside the study team.
If you have questions, please contact Dr. Caitlin Scott at caitlin.scott@educationnorthwest.org or 1.800.547.6339 x585.
Thank you for your participation!
Per the policies and procedures required by the Education Sciences Reform Act of 2002, Title I, Part E, Section 183, responses to this data collection will be used only for statistical purposes. The reports prepared for this study will summarize findings across the sample and will not associate responses with a specific district or individual. We will not provide information that identifies you or your district to anyone outside the study team, except as required by law. Any willful disclosure of such information for nonstatistical purposes, without the informed consent of the respondent, is a class E felony. The survey is proprietary and approval by the federal Office of Management and Budget (OMB) does not imply endorsement by the Department of Education.
Background
What month did you assume your current position as principal of your school? Please check one response in the box below the appropriate month.
Jan |
Feb |
March |
April |
May |
June |
July |
Aug |
Sept |
Oct |
Nov |
Dec |
|
|
|
|
|
|
|
|
|
|
|
|
What year did you assume your current position as principal of your school?
Year you became principal at your school:________________
Are you familiar with implementation of the SIG-funded transformation model at your school?
Yes (GO to QUESTION 4)
No
IMPORTANT NOTE: If you are not familiar with implementation of the SIG-funded transformation model at your school, we would appreciate it if you would please provide the name, title, email address, and phone number of someone whom you believe is familiar with SIG implementation, such as:
The former principal of your school who was involved in the implementation of the SIG-funded transformation model
A district administrator responsible for school improvement
A school-level administrator, such as an assistant principal, who was involved in the implementation of the SIG-funded transformation model at your school
A teacher who had responsibilities for assisting in the implementation of the school’s SIG-funded transformation model
-
Name
Title
Email address
Phone number (including area code)
Implementation of the Transformation Model
To what degree has your school implemented each of the following activities related to the SIG transformation model? For each of the following transformation activities, please check the first box if your school was not planning to implement that particular transformation activity; check the second box if your school is planning and preparing to implement that activity but has not yet done so; check the third box if your school has partially implemented the activity; or check the fourth box if your school has fully implemented the activity. Please check ONE response for each row.
|
Implementation Stage |
|||
Transformation Activity |
N/A (not intending to implement) |
Planning/ developing (planning and preparing to implement this activity) |
Partially implemented (actively implementing this activity, but some aspects are not yet completely integrated into routines) |
Fully implemented (completely implemented this activity, which is now a routine part of our school) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Among the transformation activities that are fully implemented in your school, which of the following, if any, do you believe were essential to your core efforts to improve your school?
(Check ALL that apply.)
Transformation Activity |
Essential to core school improvement efforts |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In addition to activities associated with the transformation model, has your school implemented any other school improvement activities during the SIG funding period (i.e., academic years 2010/11 through 2013/14)?
Yes
No (GO to question 7)
Don’t know/can’t remember (GO to question 7)
If “yes,” please list any additional school improvement activities your school implemented during the SIG funding period.
_____________________________________________________________________________________
_____________________________________________________________________________________
Did any of the following factors act as barriers to your school’s capacity to implement a particular transformation activity? Please indicate whether insufficient funding, staff expertise, staff time, technological capacity/equipment, teacher support, or district support/guidance acted as a barrier to your school’s capacity to implement each of the following transformation activities. Check all that apply.
|
Challenge |
|||||||
Transformation Activity |
N/A: No challenge |
Insufficient funding |
Insufficient staff expertise |
Insufficient staff time |
Insufficient technological capacity/ equipment |
Insufficient teacher support |
Insufficient district support/ guidance |
Don’t know |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please specify whether any OTHER factors acted as barriers to your school’s capacity to implement each of the following transformation activities.
Transformation Activity |
Other Factors |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Technical Assistance that Supports Implementation of
Transformation Activities
Please indicate the extent to which you agree that the technical assistance your school received from your school district on each of the following SIG transformation activities was sufficient. If your school district did not provide technical assistance, please select “not applicable.” (Check ONE response for each row.)
Transformation Activity |
The technical assistance provided by my SCHOOL DISTRICT on this topic was sufficient. |
||||
Strongly disagree |
Disagree |
Agree |
Strongly agree |
Not applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
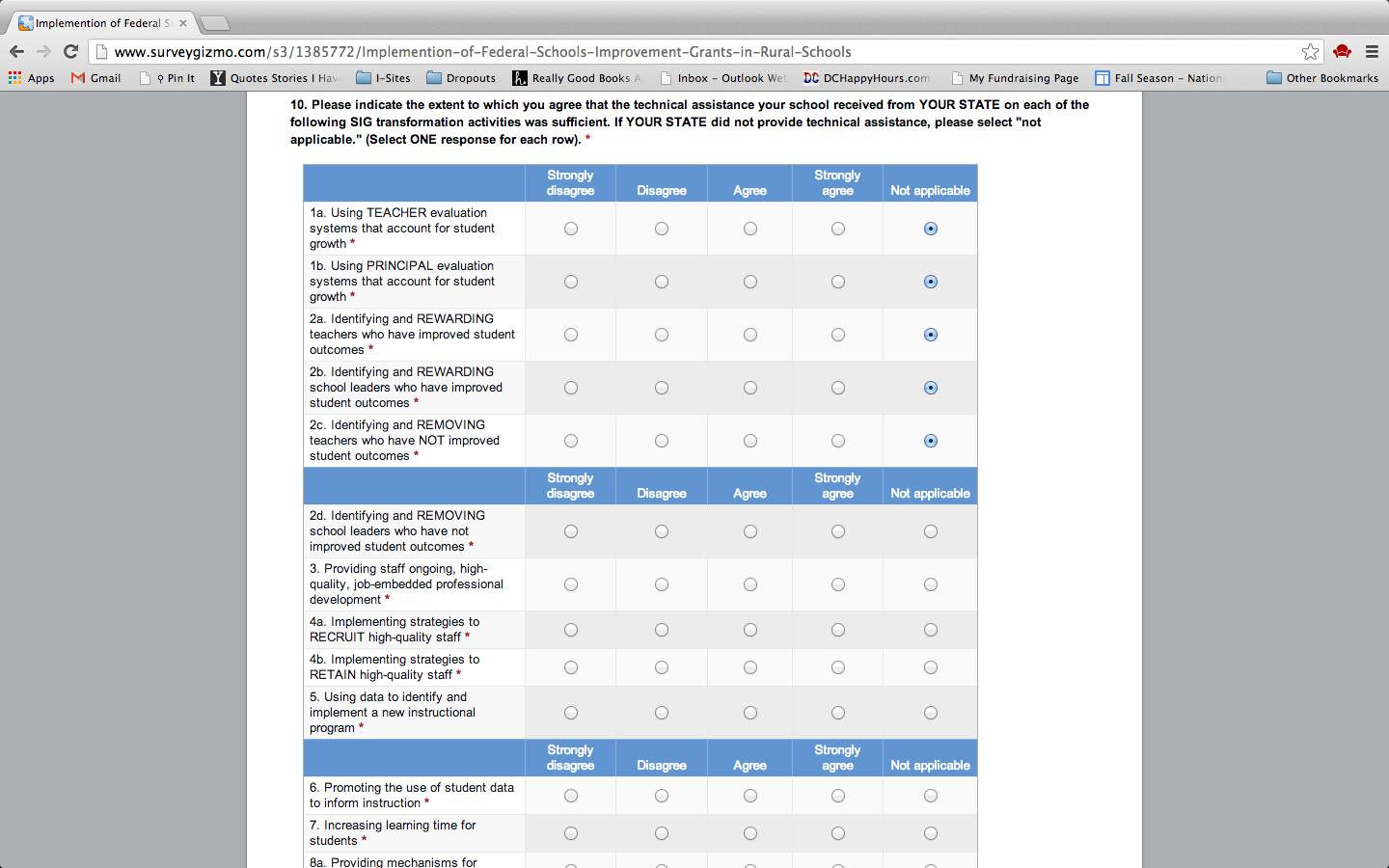
Please indicate the extent to which you agree that the technical assistance your school received from your state on each of the following SIG transformation activities was sufficient. If your state did not provide technical assistance, please select “not applicable.” (Select ONE response for each row.)
Transformation Activity |
The technical assistance provided by my STATE was sufficient. |
||||
Strongly disagree |
Disagree |
Agree |
Strongly agree |
Not applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
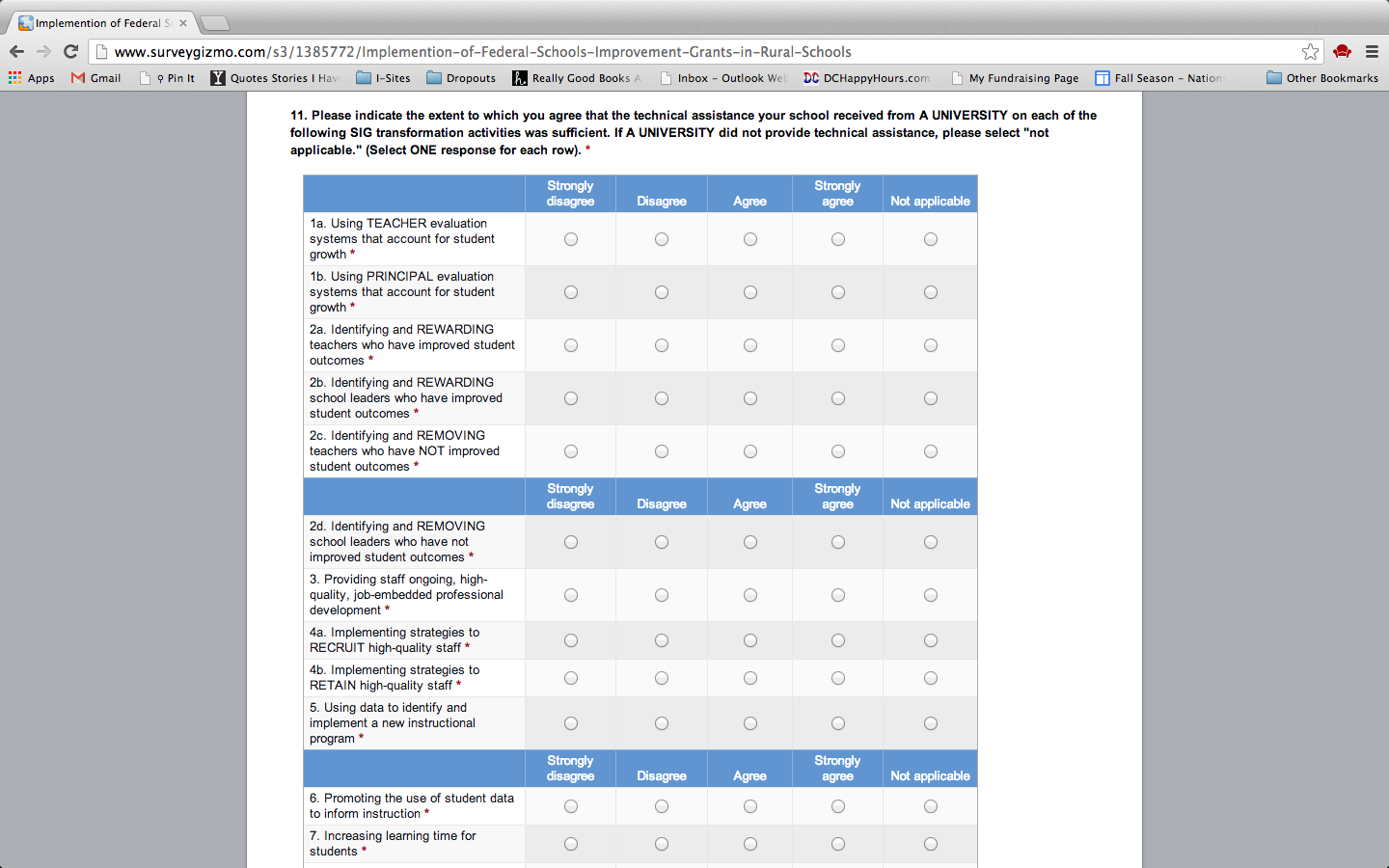
Please indicate the extent to which you agree that the technical assistance your school received from a university on each of the following SIG transformation activities was sufficient. If a university did not provide technical assistance, please select “not applicable.” (Select ONE response for each row.)
Transformation Activity |
The technical assistance provided by a UNIVERSITY was sufficient. |
||||
Strongly disagree |
Disagree |
Agree |
Strongly agree |
Not applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
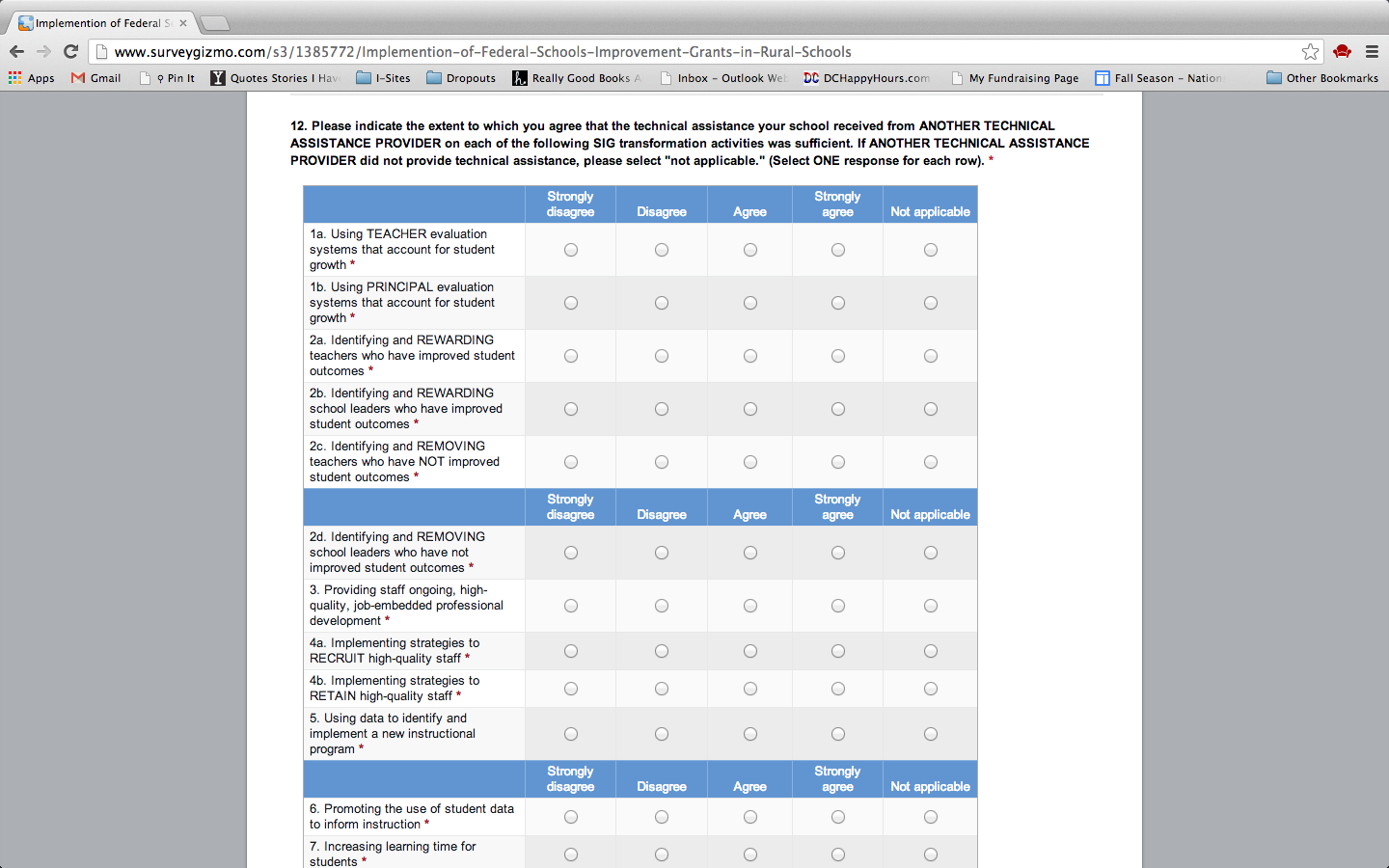
Please indicate the extent to which you agree that the technical assistance your school received from another provider on each of the following SIG transformation activities was sufficient. If another provider did not provide technical assistance, please select “not applicable.” (Select ONE response for each row.)
Transformation Activity |
The technical assistance provided by ANOTHER PROVIDER was sufficient. |
||||||
Strongly disagree |
Disagree |
Agree |
Strongly agree |
Not applicable |
|||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider: ______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
||
Transformation Activity (CONT.) |
The technical assistance provided by ANOTHER PROVIDER was sufficient. |
|||||
Strongly disagree |
Disagree |
Agree |
Strongly agree |
Strongly disagree |
||
Please specify the technical assistance provider:
_____________________________________________ |
|
|
|
|
|
|
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
|
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
|
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
|
Please specify the technical assistance provider:
______________________________________________ |
|
|
|
|
|
|
Thank you for taking our survey. Your response is very important to us.
Screen Shots of Online Survey






| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | 001001 |
| File Modified | 0000-00-00 |
| File Created | 2021-01-28 |
© 2026 OMB.report | Privacy Policy