Form 56 Home Healthcare for Healthcare Providers
Medical Expenditure Panel Survey - Household and Medical Provider Components
Attachment 56 -- Home Healthcare for Healthcare Providers
Home Care Providers Event Form
OMB: 0935-0118
MEDICAL EXPENDITURE PANEL SURVEY
MEDICAL PROVIDER COMPONENT
EVENT FORM
FOR
HOME CARE - HEALTH CARE PROVIDERS
FOR
REFERENCE YEAR 2022
Specifications for RCD
Version # |
Generation of changes |
date to AHRQ |
1.0 |
Updates made for 2022 data collection – highlights in yellow |
12/20/22 |
|
|
|
|
|
|
|
|
|
PROGRAMMERS: This document details the specifications for the Home Care-Health Care Providers Medical Event Form.
Overall functionality requirements we would like for the system controlling the event forms are as follows:
Show an “overall” progress indicator on the screen.
Set up FUNCTION KEYS for each of the following commands:
Don’t Know
Refused
The function keys would be available for any question unless specified otherwise in the question by question specifications.
NOTE: 2018 Update: The response option of “Retrievable” was removed from all Event Forms.
To assist the DCS/abstractors if they need to jump around a form, among forms, and among patients for a given provider:
Within an event form, in addition to post-logic, include pre-logic to the area we are skipping to, so the interviewer wouldn’t be able to access a group of questions without answering the gateway question. For example, the “Capitated Basis” section should not allow entry unless the question in “Reimbursement Type” (C3) = 2.
Incorporate edit trails (e.g., if need to go back and revise answer).
Include in the screen header some sort of progress status on how many patients for a given provider have been completed out of the total (e.g., Done with 2 of 3 patients).
Allow the DCS/abstractors to see a list of the event forms completed for a given patient (with event dates) in case they need to go back to revise some information in one of the forms.
Once the DCS/abstractors finish with one patient they are taken back to a summary screen listing all patients for that provider, so they can click on the next patient.
Question By Question Specifications
The QxQ specifications have been broken out throughout the rest of this document by section and include the screen layout, programmer notes, and edit specifications from Westat.
NOTE 1:
The variable names have been included where radio buttons or text boxes should appear. The variables in RED FONT were new for base year (2009). The variables in GREEN FONT were new for Option Year 1 (2010). The variables in PURPLE FONT are new for Option Year 2 (2011). The variables in BLUE FONT are those that were used by WESTAT.
NOTE 2:
Items requiring integration with the call center case management system (see items in PINK FONT) are still pending.
NOTE 3: Westat EDIT SPECS:
Westat editors wrote BLUE SHEETS to the TRC (telephone research center) for data items that needed collection, clarification, or correction. The TRC is our contact with the respondent in the provider’s office.
Westat editors wrote YELLOW SHEETS for problematic items that needed managerial review.
NOTE 4:
The following are a list of CRITICAL ITEMS and ADDITIONAL DATA RETRIEVAL ITEMS in the event form, which were pulled from (1) the CHEAT SHEET provided by AHRQ with the edit specs (cheat sheet rev2 DRG after 10-1-07.doc found in \\rtints27\meps\00_Admin\04_Documents\Materials From AHRQ and Westat\11_14_2008\Docs_Received_Electronically\MPC_Edit_Specx.zip) and (2) the following memo \\RTINTS27\MEPS\01_BASE_YEAR\11_DATA_COLLECTION\00_DCT_COMMON\REQUESTS_FOR_CLIENT\FROM CLIENT\CRITICAL DATA ITEMS MEMO 01051997.PDF.
CRITICAL ITEMS
DATE OF VISIT
At least month and year must be recorded.
SERVICES PROVIDED (review event type)
FOR Home Care (Health) – At least one type of home care personnel must have hours or number of visits
OR Durable Medical Equipment Only must be checked. At least one procedure code or description must be recorded.
REIMBURSEMENT
Fee for service or capitated must be circled.
SOURCE OF PAYMENTS
The amount paid by each source must be recorded, OR the total payments and the contributing source must be recorded. This includes OTPAYMOS and OTPAYMOSTXT.
OMB SECTION
dcs: in general, presss <F6> for don’t know AND <F7> FOR REFUSAL. AT ANY POINT, PRESS <f2> FOR SHORTCUT TO ALL DK/RF RESPONSES. USE UP/DOWN ARROWS OR PAGE UP/DOWN TO MOVE THROUGH RESPONSES. PRESS END BUTTON TO JUMP TO THE LAST OPEN QUESTION.
READ THIS ALOUD ONLY IF REQUESTED BY RESPONDENT.
OMB Statement:
Public reporting burden for this collection of information is estimated to average 3 minutes per response, the estimated time required to complete the survey. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: AHRQ Reports Clearance Officer Attention: PRA, Paperwork Reduction Project (0935-0118) AHRQ, 5600 Fishers Lane, Rockville, MD 20857.
OMB No. [#]; Exp. Date [DATE]
CONTINUE
BILLING
[BILLING (1 of 1)]
ScreeN LAYOUT
Did you bill for the services provided in (PATIENT NAME)’s home during calendar year [FILL_YR] by month, or by 60-day period?
By month; = 1 R_HOWBILL
By 60-day period = 2
BY SOME OTHER PERIOD (USE THIS RESPONSE
ONLY IF PROVIDER ABSOLUTELY CANNOT
CALCULATE COSTS BY MONTH)? = 3
(IF SOME OTHER PERIOD: What was that?) OTHBILL
PROGRAMMER NOTES
(PATIENT NAME) should fill with patient’s first name and patient’s last name from Housing Component data file.
OTHBILL - ALLOW 50 CHARACTERS
DK/REF NOT ALLOWED FOR R_HOWBILL; DK/REF ALLOWED FOR OTHBILL – CONTINUE TO E1
EDIT SPECS FROM WESTAT
NONE – This is a new question for 2009
VISIT DATE
[Page 3 – VISIT DATE (1 of 1)]
ScreeN LAYOUT
E1. During calendar year [FILL_YR], what (was the (first/next) month/ (was the begin / was the end date) of the (first/next) 60-day period/ (was the begin / was the end) date of the (first/next) OTHER PERIOD) during which your records show that home care services were provided to (PATIENT NAME)?
REFERENCE PERIOD – CALENDAR YEAR [FILL_YR]
DCS: ENTER A DATE IN FORMAT MM/DD/YYYY. INCLUDE LEADING 0’s FOR SINGLE DIGIT MONTHS AND DAYS.
|
MONTH: EVNTBEGM / EVNTBEGY MONTH YEAR OR
BEGIN DATE: R_EVNTBEG_D MM/DD/YYYY
END DATE: R_EVNTEND_D MM/DD/YYYY
|
PROGRAMMER NOTES
(was the (first/next) month/ (was the begin/was the end) date of the (first/next) 60-day period/ (was the begin/was the end) date of the (first/next) OTHER PERIOD) -
IF R_HOWBILL=1, fill: “was the (first/next) month”
If first event form for patient fill: “first” ELSE fill: “next”.
IF R_HOWBILL=2, fill “was the begin / was the end date of the (first/next) 60-day period”
If first event form for patient fill: “first” ELSE fill: “next”.
Use “was the begin” fill for R_EVNTBEG_D. Use “was the end” fill for “R_EVNTEND_D
IF R_HOWBILL=3, fill “was the begin / was the end date of the (first/next) OTHER PERIOD.
If first event form for patient fill: “first” ELSE fill: “next”.
Fill OTHER PERIOD with text from OTHBILL.
Use “was the begin” fill for R_EVNTBEG_D. Use “was the end” fill for “R_EVNTEND_D
(PATIENT NAME) should fill with patient’s first name and patient’s last name from Housing Component data file.
IF R_HOWBILL=1 ONLY ALLOW A RESPONSE TO “MONTH” (EVNTBEGM).
IF R_HOWBILL=(2 or 3) ONLY ALLOW A RESPONSE TO “BEGIN DATE” (R_EVNTBEG_D) AND “END DATE” (R_EVNTEND_D).
EVNTBEGM – value for month should be between 1 and 12
R_EVNTBEG_D – value for month (MM) should be 1 through 12; value for day (DD) should only valid numbers (1-28 for all months; 29-30 for all months except month 2; 31 allowed only for months 1, 3, 5, 7, 8, 10, and 12; value 29 allowed for month 2 only in leap years); value for year (YYYY) should be 2021 or 2022.
R_EVNTEND_D – value for month (MM) should be 1 through 12; value for day (DD) should only valid numbers (1-28 for all months; 29-30 for all months except month 2; 31 allowed only for months 1, 3, 5, 7, 8, 10, and 12; value 29 allowed for month 2 only in leap years); value for year (YYYY) should be 2022 or 2023.
IF R_EVNTBEG_D YEAR (YYYY) = 2021, R_EVNTEND_D YEAR (YYYY) MUST BE 2022
IF R_EVNTEND_D YEAR (YYYY) = 2023, R_EVNTBEG_D YEAR (YYYY) MUST BE 2022
DK/REF – CONTINUE TO E2
EDIT SPECS FROM WESTAT
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
E1 – Month/year event took place
Date must be given as Month and Year.
Blue Sheet, if month is missing and not DK or RF.
Convert month to its two-digit numeric equivalent. Circle it
DK or RF is acceptable for month. DK or RF must be verified for year.
If DK, change to –8.
If RF, change to –7.
If date is DK or RF, Blue Sheet asking if at least the year can be determined
Year must be 2022.
Books may be created for 2021 or 2023 dates if they are part of a lump that includes 2022 events. Thesebooks will be deleted after the lump payment is calculated.
Blue Sheet, if year is not 2022, cannot be determined to be 2022, and is not part of a lump that includes 2022 events.
Change year to 2022, if wrong, but book is in the middle of a series of books in 2022.
DIAGNOSES
[Page 4 – DIAGNOSES (1 of 1)]
ScreeN LAYOUT
E2. I need to know the diagnoses for (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE)). I would prefer the ICD-10 codes or DSM-5 codes, if they are available. IF CODES ARE NOT USED, RECORD DESCRIPTIONS. RECORD UP TO FIVE ICD-10 CODES OR DESCRIPTIONS.
Any more diagnoses?
|
ICD-10 CODE DESCRIPTION ICDCND# ICDPDS# ICDCND# ICDPDS# ICDCND# ICDPDS# ICDCND# ICDPDS# ICDCND# ICDPDS#
|
PROGRAMMER NOTES
[SYSTEM WILL ALLOW FOR A MAXIMUM OF 5 ICD-10 CODES AND/OR DESCRIPTIONS TO BE COLLECTED]
This is a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the questions that reads: Any More Diagnoses? YES=1 NO=2
(PATIENT NAME) should fill with patient’s first name and patient’s last name from Housing Component data file.
(during (MONTH)/from (BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “during (MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_EVNTEND_D from E1
ICDPDS# ALLOWS UP TO 100 CHARACTERS.
DK/REF – CONTINUE TO E3
For ICDCND, display “ENTER CODE” on screen. For ICDPDS, display “ENTER DESCRIPTION” on screen.
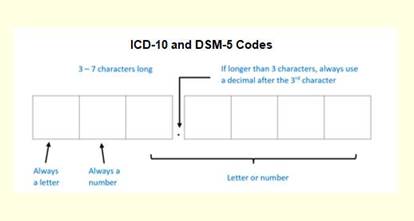
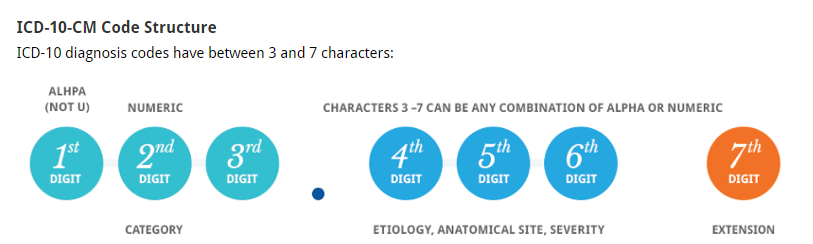
2019 UPDATE: Addition of onscreen ICD-10 graphic to emphasize correct code format. Logic also added to restrict code entries to only accurate formats.
Code is 3-7 characters.
First character is always a letter.
Second character is always a number.
Characters 3-7 can be letter or number.
2020 UPDATE: Values entered into ICDCND are checked against a dictionary of valid ICD-10 and DSM-5 codes. Entry is allowed for valid codes. If entry of an invalid code is attempted, a hard check message is displayed, “The code you entered is not in our database. Please verify your entry. If the entry is correct, leave ICDCND empty and move to ICDPDS field to enter a description instead.”
EDIT SPECS FROM WESTAT
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
QE2 – Diagnosis
CRITICAL ITEM
USED FOR DETERMINING SBDs
Must have at least one Diagnosis, in text or code.
Blue Sheet.
DK and RF are acceptable answers.
Change DK to –8. Change RF to –7.
Code PL-IV as 60, critical item is DK or RF.
If one Diagnosis is given and another is DK, cross out the DK and keep the Diagnosis given.
Diagnosis descriptions must be valid, clear, and legible.
Blue Sheet
Diagnosis descriptions may be the identification of a disease or illness.
Symptoms are acceptable for Diagnosis.
Procedures are acceptable for Diagnosis.
Accept the name of a disease.
Accept symptoms such as cough or nausea.
Accept procedures such as lab work, screening mammogram, flu shot, employment physical, or school physical.
Do not accept “Follow-up” without any other information. Blue Sheet, asking Follow-up for what.
Abbreviations in the Description field should be standard medical abbreviations.
Review abbreviations.
Check reference list in manual.
Check medical dictionary.
Ask team leader to check website.
Yellow Sheet, if not found, and team leader is not available.
There should be only 1 diagnosis per line.
If there are 5 or more codes, the order of the codes must be maintained.
Change
To
Change
To
650 652
V27.1
V25.2
V25.09
650
652
V27.1
V25.2
V25.09
650 652
V27.1
V25.2
650
V27.1
V25.2
652
If two codes are listed on the same line, rewrite one of the codes.
If there are 4 or less Diagnoses, write the code on the last line.
If there are 5 or more Diagnoses, write the code on the next line and rewrite all other codes, keeping them in order.
The code field and the description field cannot be used on the same line.
CODE DESCRIPTION
650
Normal Delivery
A mixture of codes and descriptions are acceptable if they are on different lines.
CODE DESCRIPTION
650 _____________
____ Normal Delivery
Look up the diagnosis code in the ICD-10 reference book.
If they are on the same line, and the code’s definition exactly matches the text description, cross out the text and keep the code. Do not look up codes if they are on different lines.
If there are 5 or more Diagnoses, write the code on the next line and rewrite all other codes, keeping them in order
A diagnosis may only appear in the book once.
Note: different numbers after the decimal mean that a diagnosis is not a duplicate. Keep both.
547.11 and 547.1 are not duplicates
698 and 698.0 are not duplicates
Cross out a duplicate diagnosis.
Descriptions cannot go over 100 characters.
Take to a team leader to shorten, or write a Yellow Sheet, if a team leader is not available.
Some sequential events will have ongoing treatments for a condition.
Pre-natal care
Dialysis
Physical or Occupational Therapy
If diagnosis is given in some books, but DK or RF in other books, managerial review is needed.
Yellow Sheet, if diagnosis is given in some books, but is DK or RF in other books.
Diagnosis Counter
Office Use Only box must be filled in.
The Office Use Only box is only used on the booklet page, not on the Continuation Sheet.
Count the number of diagnoses and enter as a 2-digit, zero-filled number.
Diagnosis of DK or RF = Diagnosis count of 01.
CHEAT SHEET RANGES FOR DIAGNOSES (ICD-10)
Codes are between 3 and 7 characters, ranging from A00 to Z99.
SERVICES/CHARGES
NOTE: See end of section for edit specs from Westat for questions E3, E4, C1a, C1b, and C2.
[Page 5 – SERVICES/CHARGES (1 of 4) ]
ScreeN LAYOUT E3. I need to know which types of home care personnel provided care to (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE)) and either the number of hours or the number of visits for each type. EXPLAIN IF NECESSARY: By type of person I mean a housekeeper, therapist, nurse aide, yard worker, and so forth.
E3PERS# Which type of home care personnel provided care to (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE))?
SELECT ONE
EXPLAIN IF NECESSARY: By type of person I mean a housekeeper, therapist, nurse aid, yard work
How many VISITS for [FILL PERSON TYPE SELECTED AT PERSTYPE]?
HIT ENTER/LEAVE EMPTY IF ENTERING NUMBER OF HOURS.
How many HOURS for [FILL PERSON TYPE SELECTED AT PERSTYPE]?
How many MINUTES for [FILL PERSON TYPE SELECTED AT PERSTYPE]?
|
E3_LEADIN
PERSON TYPE VISITS HOURS MINUTES PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN# PERSTYPE# PERSVS# OR PERSHR# PERSMN#
PERSVS#
PERSHR#
PERSMN#
|
|
|
[Page 5 – SERVICES/CHARGES (2 of 4)
ScreeN LAYOUT
E4. I need the services provided (during (MONTH)/from (BEGIN DATE) through (END DATE)). I would prefer either the CPT-4 codes or the revenue codes, if they are available.
RECORD CPT-4 CODE OR REVENUE CODE. IF CODES ARE NOT USED, RECORD DESCRIPTION OF SERVICES AND PROCEDURES PROVIDED.
IF ENTERING A CPT-4 CODE, ENTER UP TO 8 CHARACTERS. IF CPT-4 CODE BEGINS WITH W, X, Y OR Z, ENTER A DESCRIPTION INSTEAD.
HIT ENTER/LEAVE EMPTY IF ENTERING REVENUE CODE OR DESCRIPTION.
Any more services?
|
CPT-4 CODE REVENUE CODE DESCRIPTION MCPT# MREVCD# MCPTDS# MCPT# MREVCD# MCPTDS# MCPT# MREVCD# MCPTDS# MCPT# MREVCD# MCPTDS# MCPT# MREVCD# MCPTDS# MCPT# MREVCD# MCPTDS# |
PROGRAMMER NOTES
2020 UPDATE: Values entered into MCPT are checked against a dictionary of valid CPT-4 and HCPCS codes. Entry is allowed for valid codes. If entry of an invalid code is attempted, a hard check message is displayed, “The code you entered is not in our database. Please verify your entry. If the entry is correct, leave MCPT empty and move to MCPTDS field to enter a description instead.”
2022 UPDATE: Modifiers added in MCPT must be 2 characters. After the first 5 characters in an MCPT field, any additional entry within that same field must be 0 characters or 2 characters.
2016 UPDATE: REQUESTING EVENT FORM CHANGE IN WHAT IS CONSIDERED AN ERROR FOR E4 GRID. [The following only occurs during re-abstraction: If an event includes a duplicated CPT code and associated charge that needs to be deleted, the deletion creates errors for all CPTs/charges listed after it, even if their CPTs or values do not change. This happens when the deleted item is not the last in the list/grid. For example, if the second CPT and associated charge in the list is deleted, the system marks that removal as an error. Then it shifts every CPT and charge “below” that one in the grid. Each one of those shifts counts as an error. Requesting Event Form change in what is considered an error.]
E4 - [SYSTEM WILL SET UP AS A LOOP, SO NO LIMIT ON CPT-4 CODES REQUIRED]
E4 – place the text box for revenue code between the CPT-4 code and the description.
E4 – Permit users to enter CPT-4 or revenue code, but not both. Error message, “Enter CPT-4 or Revenue Code, not both.”
E3 - (PATIENT NAME) should fill with patient’s first name and patient’s last name from Housing Component data file.
E3 and E4 - (during (MONTH)/from (BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “during (MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_EVNTEND_D from E1
E3 – Data may be entered for “Hours/minutes” OR “Visits”, NOT BOTH
E3 – DECIMALS ARE NOT ALLOWED
E3(15) - This is a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the questions that reads:
Any more types of home care personnel? YES=1 NO=2
E4 - This is a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the questions that reads: ANY MORE SERVICES? YES=1 NO=2
E4 - MCPTDS# allows up to 100 characters.
E3 - DK/REF – CONTINUE TO E4
E4 – DK/REF – CONTINUE TO C1a
E3 - There is a loop of 10 items in the order of:
PERSTYPE# PERSVS# OR PERSHR# PERSMN# E3_AnyMore# ("Any more types of home care personnel?")
The items in this loop correspond/get calculated to the list of variables in the table below, which are specific to personnel type for output purposes.
HOURS/MINUTES VISITS
1. Home Health Aide HHAIDHR / HHAIDMN OR HHAIDVS
2. Homemaker HMAKEHR / HMAKEMN OR HHMAKEVS
3. I.V./Infusion
TherapIST IVTHERHR / IVTHERMN OR IVTHERVS
4. Nurse/
Nurse Practitioner NURSEHR / NURSEMN OR NURSEVS
5. Nurse’s Aide NURAIDHR / NURAIDMN OR NURAIDVS
6. Occupational
Therapist OCCTHHR / OCCTHMN OR OCCTHVS
7. Personal Care
Attendant PERCARHR / PERCARMN OR PERCARVS
8. Physical Therapist PHYSTHHR / PHYSTHMN OR PHYSTHVS
9. Respiratory
Therapist RESPTHHR / RESPTHMN OR RESPTHVS
10. Social Worker SOCWRKHR / SOCWRKMN OR SOCWRKVS
11. Speech Therapist SPECTHHR / SPECTHMN OR SPECTHVS
12. YARD WORKER R_YARDWKHR / R_YARDWKMN OR R_YARDWKVS
13. DRIVER R_DRIVERHR / R_DRIVERMN OR R_DRIVERVS
14. BABYSITTER R_BABSITHR / R_BABSITMN OR R_BABSITVS
15. Any other home care personnel?
R_OTHHCR OTHHCRHR / OTHHCRMN OR OTHHCRVS
E3 – R_OTHHCR: Specify the other home care personnel.
E3 – R_OTHHCR allows up to 100 characters.
E3 – When 2 is entered for E3_AnyMore#, run soft check. If one or more individual entry for hours (PERSHR#) is greater than 500, display soft check: You have reported over 500 hours. Please review and correct if needed, or suppress and continue.
E3 – Range for visits (PERSVS#) = 0-999. Range for hours (PERSHR#) = 0-999. Range for minutes (PERSMN#) = 0-59.
[Page 6 – SERVICES/CHARGES (3 of 4)]
ScreeN LAYOUT
C1a. Could you tell me the full established charges -- before any adjustments or discounts -- for all services provided by home care personnel (during (MONTH)/from (BEGIN DATE) through (END DATE)).
EXPLAIN IF NECESSARY: This would be the charges for the (READ TYPES OF PERSONNEL FROM E3 ABOVE) who provided services (during (MONTH)/from (BEGIN DATE) through (END DATE)).
EXPLAIN IF NECESSARY: The full established charge is the charge maintained in the organization’s billing system for billing insurance carriers and Medicare or Medicaid. It is the “list price” for the service, before consideration of any discounts or adjustments resulting from contractual arrangements or agreements with insurance plans.
IF NO CHARGE: Some organizations that don't charge on the basis of services provided do associate dollar amounts with services for purposes of budgeting or cost analysis. This is sometimes called a "charge equivalent." Could you give me the charge equivalents for these procedures?
NOTE: WE NEVER ENTER $0 FOR A CHARGE
C1b. And could you tell me the full established charges for everything other than personnel services (during (MONTH)/from (BEGIN DATE) through (END DATE)), including durable medical equipment, drugs, supplies, and so forth?
EXPLAIN IF NECESSARY: This would include charges for anything other than the services of the home care personnel you just told me about.
IF NO CHARGE: Some facilities that don’t charge for each individual service do associate dollar amounts with services for purposes of budgeting or cost analysis. This is sometimes called a “charge equivalent”. Could you give me the total of the charge equivalents for everything other than personnel services, including durable medical equipment, drugs, supplies, and so forth?
IF THOSE COSTS WERE INCLUDED IN PERSONNEL CHARGES, RECORD 0.00.
INCLWPERSCHG IF PREVIOUS COSTS WERE RECORDED AS 0.00 BECAUSE THEY WERE INCLUDED IN PERSONNEL CHARGES, ENTER 1.
IF THERE SIMPLY WERE NO NON-PERSONNEL CHARGES (VALID 0), ENTER 0.
|
FULL ESTABLISHED CHARGES FOR: PERSONNEL SERVICES: $PERSCHRG
ALL OTHER CHARGES: $NONPCHRG
NCLWPERSCHG |
C2. I show the total of all of the full, established charges for (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE)) as [SYSTEM WILL COMPUTE AND DISPLAY TOTAL]. Is that correct?
|
TOTAL CHARGES: $TOTLCHRG
|
PROGRAMMER NOTES
C1a, C1b, and C2 - (during (MONTH)/from (BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “during (MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_EVNTEND_D from E1
C1a (READ TYPES OF PERSONNEL FROM E3 ABOVE) should fill with responses selected in E3.
C1b, IF INCLWPERSCH “INCLUDED WITH PERSONNEL CHARGES” is 1, code C1b as “-4” (see edit specs below).
C2, VERIFY – (Is this/Are these) - If there are amounts for both C1a and C1b fill: "Are these" ELSE fill: "Is this".
C2, VERIFY – (s) - If there are amounts for both C1a and C1b fill: "s" ELSE fill: " ".
C2, VERIFY – (this/these) - If E4 has one response fill: "this" ELSE fill: "these".
C2, VERIFY – (s) - If E4 has one response fill: " " ELSE fill: "s".
C2 - (PATIENT NAME) should fill with patient’s first name and patient’s last name from Housing Component data file.
C2, implement soft check of TOTLCHRG is GT 25000. Soft check reads: You have entered charges over $25,000. Please review and correct if needed, or suppress and continue.
C2 – customized wording. If there is even one reserve code entered in the charge fields, then end the currently displayed phrase with “…although one or more charges are missing.”. For example:
I show the total of all of the full, established charges for (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE)) as $600, although one or more charges are missing” Is that correct?”
If all the entries are reserve codes, then display:
I show the total of all of the full, established charges for (PATIENT NAME) (during (MONTH)/from (BEGIN DATE) through (END DATE)) as undetermined, although one or more charges are missing” Is that correct?”
C1a, C1b, and C2 - DOLLAR AMOUNTS SHOULD BE FORMATTED TO INCLUDE COMMAS and DECIMAL POINTS
C1a - DK/REF – CONTINUE TO C1b
C1b - DK/REF – CONTINUE TO C2
C2 - DK/REF – CONTINUE TO C3
C1b – If C1b NONPCHRG = 0, GO TO INCLWPERSCHG, ELSE GO TO C2.
EDIT SPECS FROM WESTAT
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
E3 – Type of personnel
Hours/min
# of visits
At least one type of home care personnel must have hours or number of visits
OR Durable Medical Equipment Only must be checked.
1 – Home Care Aide
2 – Homemaker (include Housekeeper)
3 – IV/Infusion Therapist
4 – Nurse/Nurse Practitioner
5 – Nurse’s Aide
6 – Occupational Therapist
7 – Personal Care Attendant
8 – Physical Therapist
9 – Respiratory Therapist
10 – Social Worker
11 – Speech Therapist
12 – OTHER (Specify)
21 – Yard Worker*
22 – Driver*
23 – Babysitter*
Blue Sheet if there is no personnel service given and Durable Medical Equipment Only box is not checked.
Yellow Sheet, if DK or RF.
If yard worker, driver, or babysitter is indicated, write corresponding number (e.g., 21, 22, 23).
If the answers 1-11 are given in the Other/Specify line, transfer the answer to the proper line.
If answer is 12 OTHER (Specify), check the Decision Log list at the end of the spex. If the answer is on the list, accept. If it is not on the list, Yellow Sheet.
HOURS/MINUTES column:
Hours = zero-filled 3-digit number
Minutes = zero-filled 2-digit number
Hours/Minutes should not be greater than 144/00.
If. hours and minutes are written as a decimal or fraction, use the conversion chart on the Cheat Sheet to change the answer to hours and minutes. Circle the hours and minutes as one answer.
Yellow Sheet, if more than 144 hours and minutes are recorded for one type of personnel.
VISITS column:
Zero-filled 3-digit number
Number of visits should not be greater than 93.
Convert the number to 3-digits, zero-filled. Circle the number.
Yellow Sheet, if more than 93 visits are recorded for one type of personnel.
Either Hours/Minutes or number of Visits must be filled in, but not both.
Keep the hours and minutes, and cross out the number of visits.
There should not be an answer in both personnel visits or hours and Durable Medical Equipment Only.
Durable Medical Equipment Only means that the only service was the supply of equipment: Hospital Bed, Oxygen Concentrator and tanks, etc.
Yellow Sheet.
E4 – Services
RECORD 2-digit zero-filled count of # of services
All procedure codes must be within ranges.
CPT-4 codes [Use Cheat Sheet and OBD spex]
HCPCs [Use Cheat Sheet and OBD spex]
Text Descriptions [Review for legibility, clarity]
Revenue Codes [Use Revenue Code Summary sheet]
Blue Sheet.
Be sure that the answer is in the proper column.
HCPCs should be in the CPT Code column.
If CPTs and HCPCs are written in the Revenue Center Code column, cross out and rewrite in the correct column.
If Revenue Codes are written in the CPT Code column, cross out and rewrite in the Revenue Center Code column.
Circle the column heading if there is an answer in that column.
Only one service per line.
Blue Sheet.
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
E4
PROCEDURES
PROCEDURE IS A CRITICAL ITEM
There must be at least one procedure, written as a text description, as a CPT code or as a HCPC.
Blue Sheet, if procedure is missing.
DK and RF are acceptable answers.
Change DK to –8. Change RF to –7. Give an RC code of 60 (critical item missing).
Descriptions of procedures must be clear, valid, and legible.
Blue Sheet.
Abbreviations in the Description field should be standard medical abbreviations.
Review abbreviations.
Check reference list in manual.
Check medical dictionary.
Ask team leader to check website.
Yellow Sheet, if not found, or team leader not available.
Descriptions cannot be longer than 100 characters.
Ask a team leader to shorten it or Yellow Sheet.
CPT and HCPC codes must fall within valid ranges (see Cheat Sheet).
Blue Sheet.
HCPCs cannot begin with W, X, Y, or Z because these are local codes, not national codes.
Blue Sheet, asking for text description.
CPT and HCPC Modifiers must be valid. Valid modifiers include:
2 numbers
2 letters
1 letter + 1 number
1 letter
Keep all valid modifiers.
Cross out all invalid modifiers.
Note: Modifiers with X may be a multiplication sign – see below.
Only one procedure per line.
Procedures cannot be followed by a multiplication mark
(For example: 85025 x5).
Multiplication marks should not be confused with modifiers.
Blue Sheet, saying that there can only be one procedure per line.
Only one valid modifier is acceptable for each CPT code.
Cross out the second modifier.
Modifiers must be separated from the main code by a hyphen.
Change a decimal point to a hyphen.
Multiple listings of the same procedure may need managerial review.
Yellow Sheet if the same procedure is listed more than twice.
Multiple visits may need review
Check CPT codes in the 99201–99499 range.
Accept Office Visit or OP codes w/consultation codes (if the event type is compatible).
Accept Office Visit or OP codes w/ preventive medicine codes.
Yellow Sheet multiple inpatient care codes in the same book. These may appear as initial inpatient care, subsequent inpatient care and inpatient discharge code in the same book.
Yellow Sheet multiple Office Visit or OP codes in the same book.
Procedures should be consistent with the location of the event (event type).
See “edit specs from Westat” below B5a titled “Procedures That Need Special Handling”.
Compare procedure to QB3 or to the Global Fee Main Event type.
Yellow Sheet, if not consistent.
PROCEDURES THAT NEED SPECIAL HANDLING
PROCEDURES |
Specification |
Action |
Body part with no procedure |
Body part alone is not a valid procedure. |
Blue Sheet. |
Body part with indication of Radiology |
Body parts with descriptives for Radiology are acceptable. For example, 2 views, P/A, LAT, v |
Accept. |
Abbreviations |
Standard medical abbreviations are allowed. Shorthand abbreviations are not accepted. |
Look up in list of abbreviations and in med dictionary. Let a team leader look up on a website. Yellow Sheet, if a team leader is not available. |
CPT code with description |
Should not have a code and a description on the same line. 71020 Chest X-ray |
Look up code. If the code and text match, cross out text. If code and text do not match, Blue Sheet to ask if they are one procedure or two, and to get the second charge if appropriate. |
CPT code with units |
Should not have a code and text. Cross out the text. 99284
J2001
|
Cross out text. |
CPT code with multiplication mark |
Not allowed. 71020 (x2) |
Blue Sheet, saying that there can only be one procedure per line. |
State tax |
Valid if it is not the only service in the book. No identifying information is allowed. |
Yellow Sheet, if it is the only procedure. Cross out state name, if given. |
Handling 99000 - 99002 |
Valid if it is not the only service in the book. Needs further review if used alone. |
Yellow Sheet, if it is the only procedure. |
Administrative fee |
Valid if it is not the only service in the book. Needs further review if used alone. |
Yellow Sheet, if it is the only procedure. |
Surcharge |
Needs further review if used alone. Valid if it is not the only service in the book. No identifying information is allowed. |
Yellow Sheet, if it is the only procedure. Cross out state name, or other identifying information, if given. |
Ambulance, ambulance mileage |
Needs further review. |
Yellow Sheet. |
Reports, copy of reports, insurance reports |
Valid if it is not the only service in a book. |
Yellow Sheet, if it is the only procedure. |
99080 S9981, S9982 |
Valid if it is not the only service in a book. |
Yellow Sheet, if it is the only procedure. |
Rxpickup; Pharmacy |
Valid if it is not the only service in a book. |
Yellow Sheet, if it is the only procedure. |
Canceled appointment, no show charge |
Needs managerial review. |
Yellow Sheet. |
Follow up, no charge |
We take charge equivalents. |
Blue Sheet. Is this part of the Global Fee? If not, can we get a Charge Equivalent? |
Service with no charge or comment that Dr did not charge. |
We take charge equivalents. |
Blue Sheet, asking for a Charge Equivalent. |
99024 (Follow-up visit included in a Global Fee) |
A Global Fee f/u visit should appear as a GF date in the book with the main GF charge, not as a separate book. |
Blue Sheet. Should this be part of a global fee? |
99500 – 99600 (Home Care services) |
If there are Home Care services the Patient Data Form must be reviewed. Did we expect Home Care events? |
Accept, if no Home Care Events were reported on Patient Data Form. Blue Sheet if Home Care events were reported, asking that they be collected. |
Delivery 59400 – 59412, 59510-59525, 59610 – 59622 |
Valid for HS event. Verification needed for MV, OP, or ER. |
Blue Sheet to verify that event took place in physician’s office or OP dept or ER. |
Neonatal inpatient care 99295 – 99299, 99433, 99436 |
Valid for HS event. Verification needed for MV, OP, or ER. |
Blue Sheet to verify that event took place in physician’s office or OP or ER. |
Surgeries in Physician’s Office |
Surgeries may be acceptable in an MV event, depending on the complexity of the surgery and the type of physician’s office.
Providers that are Eye Centers or Surgi-Centers can do surgeries on an outpatient basis. |
Look up CPT codes, or ask a team leader.
If surgery is $1000.00 or less, and can be done on an outpatient basis, accept. If surgery is more than $1000.00, Yellow Sheet. If any questions, Yellow Sheet. |
Procedure doesn't match the location given. |
Compare QB3 to QB5a for the type of service and the location of the service (event type). |
Yellow Sheet, if procedure doesn't match event type. |
Text description says Office Visit but not an MV or OP event. |
Expect that an Office Visit would occur as an event in the Physician’s Office or in a Hospital Outpatient setting. |
Yellow Sheet if the procedure is written as “Office Visit” but event is ER or HS. |
Inpatient event with CPT codes for Path and/or Rad services. |
Office-Based cases should not have the hospital charges. |
Yellow Sheet. |
Inpatient event with room charge, or room and board, or supplies |
Office-Based cases should not have the hospital charges. |
Yellow Sheet. |
Proc is DK or RF / Charge is DKor RF/ Payments are DK |
If procedures and charges and payments are DK or RF, book needs managerial review. |
Yellow Sheet. |
CHEAT SHEET RANGES FOR PROCEDURES (CPT-4 and HCPC)
[Modifiers are separated by a hyphen – may be 2 numbers or 2 letters, a number and a letter, or one letter.]
CPT4 – 5 DIGITS:
Anesthesiology
00100 to 01999, 99100, 99116, 99135 & 99140
Surgery
10021 - 19499
20000 - 29999
30000 - 39599 (36400 - 36425 are not surgery)
40490 - 49999
50010 - 59899 (59020 & 59025 are not surgeries)
60000 - 69990
93501 - 93545, 93580 - 93581
Radiology
70010 - 79999
938_ _, 939_ _
Pathology and Laboratory
80048 - 89356
36400 - 36425, 36540
also HCPC G0001
Medicine
90281 - 99602 [HH = 99500 – 99602]
Evaluation and Management
99201 - 99499 [ER = 99281 – 99288)
HCPC – ‘ALPHA’ + 4 DIGITS STARTING WITH A, B, C, D, E,G, H, J, K, L, M, P, Q, R, S, T, V
[Do not accept W, X, Y, Z – Blue Sheet for text description]
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
C1a – Charge for Personnel Services
If there is an answer in QE3 indicating that there were personnel services, there must be a charge.
Blue Sheet.
$0.00 is acceptable if there are no personnel visits or hours and Durable Medical Equipment Only box is checked.
Accept if there were no personnel services.
DK or RF is acceptable.
Change DK to –8.
Change RF to –7.
Spex for full established charges and charge equivalents are the same as OBD.
Review charges using OBD guidelines.
C1b – Charge for Non-Personnel Services
Cannot be blank.
Write $0.00 if blank and Personnel charges = Total charges, unless there is an indication that charges are included in personnel charges.
If note says that the Non-personnel charges are included in the personnel charges, this must be indicated.
Code as –4, included in the line above.
DK or RF is acceptable.
Change DK to –8.
Change RF to –7.
If Durable Medical Equipment Only box is checked, then charge can’t be zero.
Yellow Sheet.
C2 - Total charges
Must equal Personnel charges + Non-personnel charges.
Yellow Sheet.
Can’t be zero.
Yellow Sheet if Total Charge = zero.
DK or RF is acceptable, if the other charge information agrees.
Change DK to –8.
Change RF to –7.
DECISION LOG for QE3
HOME CARE DECISION LOG FOR PERSONNEL TYPES
QE3 in HEALTH CARE PROVIDER BOOKLETS
QD2 IN NON-HEALTH CARE PROVIDER BOOKLETS
The following personnel have been approved as an answer to QE3 or QD2, type of personnel providing service in a Home Care case:
ACTIVITIES OF DAILY LIVING TRAINER
ADULT DAY CARE
BEHAVIORAL HEALTH SPECIALIST, COORDINATOR
BEREAVEMENT COUNSELOR, GRIEF COUNSELOR
CASE MANAGER
CHAPLAIN
CHILD DEVELOPMENT SPECIALIST
CNA, CERTIFIED NURSE ASSISTANT
COMPANION
COUNSELOR
CUSTODIAL CARE
DEVELOPMENTAL REHAB or THERAPIST or SPECIALIST
DIETICIAN
EARLY CHILDHOOD SPECIAL EDUCATION TEACHER
FAMILY MEMBER
HOSPICE CARE
IN HOME SUPPORT PERSON
INDEPENDENT LIVING SKILLS THERAPIST
INTAKE SPECIALIST
IV / INFUSION THERAPIST
LAB TECH
LICENSED MARRIAGE & FAMILY THERAPIST
LICENSED VOCATIONAL NURSE
MASSAGE THERAPIST
MENTAL HEALTH THERAPIST
MOBILE THERAPIST
NUTRITIONIST
PASTOR
PHLEBOTOMIST
PHYSICIAN
PODIATRIST
PSYCHOLOGIST
RESPIRATORY THERAPIST
RESPITE WORKER or RESPITE CAREGIVER
SERVICE COORDINATOR
SOCIAL TRANSPORT
SPECIAL EDUCATION TEACHER
SPIRITUAL COUNSELOR
SUPPORT STAFF, CONSUMER-DIRECTED
THERAPEUTIC STAFF SUPPORT
WOUND CARE SPECIALIST
REIMBURSEMENT TYPE
[Page 7 – REIMBURSEMENT TYPE (1 of 1)]
ScreeN LAYOUT
C3. Was your organization reimbursed for the charges (during (MONTH)/from (BEGIN DATE) through (END DATE)) on a fee-for-service basis or a capitated basis?
EXPLAIN IF NECESSARY: Fee-for-service means that the organization was reimbursed on the basis of the service provided. Capitated basis means that the patient was enrolled in a prepaid managed care plan where reimbursement is not tied to specific visits, this is also called Per Member Per Month. . IF IN DOUBT, CODE FEE-FOR-SERVICE.
|
Fee-for-service basis =1 FEEORCAP Capitated basis =2
|
PROGRAMMER NOTES
[IF FEEORCAP=2 GO TO C7a; If FEEORCAP=1 GO TO C4.]
C3 - (during (MONTH)/from (BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “during (MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_EVNTEND_D from E1
EDIT SPECS FROM WESTAT
DATA ITEM |
SPECIFICATIONS |
ACTION, if specification not met |
QC3 Fee for Service or Capitated?
CRITICAL ITEM |
1 or 2 must be circled. This critical item can usually be determined by looking at the skip pattern of the payment questions. |
If blank, answer 1 or 2, by looking at the skip pattern used for the payment questions. |
Answer must be consistent with the skip pattern used in payments section. If Fee for Service, then QC4, Box 1, and QC6 must be answered. If Capitated, then QC7a – f Capitated Section must be answered. |
If answered incorrectly, circle the answer that matches the skip pattern, and cross out incorrect response. |
|
Should be the same in all books for a patient, unless there is an explanation. |
Yellow Sheet, if there is no explanation about a change in insurance which caused the change among books. |
SOURCES OF PAYMENT
[Page 8 – SOURCES OF PAYMENT (1 of 1)] ScreeN LAYOUT
C4. From which of the following sources did your organization receive payment for the charges (for (MONTH)/from (BEGIN DATE) through (END DATE)) and how much was paid by each source? Please include all payments that have taken place between (MONTH/BEGIN DATE) and now for this care.
IF NONE, ENTER ZERO (0).
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
[DCS ONLY] IF PROVIDER VOLUNTEERS THAT PATIENT PAYS A SET DOLLAR AMOUNT FOR ALL CHARGES (DURING (MONTH)/FROM (BEGIN DATE) THROUGH (END DATE)), VERIFY: So, you receive a set dollar amount for all charges (for (MONTH)/from (BEGIN DATE) through (END DATE)) rather than payment for the specific service? IF YES: GO BACK TO FEEORCAP QUESTION (C3) AND CODE AS CAPITATED BASIS.
Any more sources?
C5. I show the total of all payments received for (MONTH) / from (BEGIN DATE) through (END DATE)) as [SYSTEM WILL COMPUTE AND DISPLAY TOTAL]. Is that correct?
|
SOURCE
a. Patient or Patient’s Family;
b. Medicare;
c. Medicaid;
d. Private Insurance;
e. VA/ChampVA;
f. Tricare;
g. Worker’s Comp; or
h. Something else? (IF SOMETHING ELSE: What was that?) OTPAYMOS OTPAYMOSTXT
TOTAL PAYMENTS
|
PAYMENT AMOUNT
$PATPAYM
$CAREPAYM
$AIDPAYM
$PINSPAYM
$VAPAYM
$CHAMPAYM
$WORKPAYM
$OTHRPAYM
$TOTLPAYM
|
PROGRAMMER NOTES
When a user answers MoreSources_1 (“Any more payments”) as “No”, and one or more entries among PATPAYM, CAREPAYM, AIDPAYM, PINSPAYM, VAPAYM, CHAMPAYM, WORKPAYM equals DK, RF administer a soft check message: “One or more charges was recorded as Don’t Know or Refused. Please review and correct if needed, or suppress and continue.”
C4 - (MONTH/BEGIN DATE)
IF R_HOWBILL=1, MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL= (2 or 3) BEGIN DATE should fill with R_EVNTBEG_D from E1
C4 - [SYSTEM WILL SET UP “SOMETHING ELSE” AS A LOOP, SO NO LIMIT REQUIRED]
C4 and C5 - (MONTH)/(BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “(MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “(BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_EVNTEND_D from E1
C4h - The OTPAYMOSTXT variable was added to record free-form text for the “Other, Specify” option. Interviewers will be able to record responses in the text box that do not occur in the listed options. Field allows up to 50 characters. Text on screen says: “Specify other payment source.”
C4h is a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the question that reads: Any more sources? YES=1 NO=2
(3) The “something else” option should be set up so a response can be selected from listed options, or entered in as text.
C4h – Include the following options in listed options for the “Other Specify”;
Auto or Accident Insurance
Indian Health Service
State Public Mental Plan
State/County/Local program
Other
C4 - DK/REF – CONTINUE TO C5
C5 - DK/REF – CONTINUE TO BOX 1
DOLLAR AMOUNTS SHOULD BE FORMATTED TO INCLUDE COMMAS and DECIMAL POINTS
Require an entry in each source of payment (SOP) field PATPAYM to WORKPAYM and OTHRPAYM. The following are allowed entries: 0, integer, integer with 2 decimal places, F6/DK, F7/REF.
C4 – OTHRPAYM – Onscreen text reads, “RECORD PAYMENT AMOUNT.”
C5 – IF RESPONSE = 2, DISPLAY HARD CHECK: “IF INCORRECT, CORRECT ENTRIES AS NEEDED.”
Design Note #1 for C5 (specifically regarding C_5OTHERPAYMENTS)
CHARGES = $[TOTLCHRG]
PAYMENTS
Patient or family $[PATPAYM]
Medicare $[CAREPAYM]
Medicaid $[AIDPAYM]
Private insurance $[PINSPAYM]
ChampVA/VA $[VAPAYM]
TRICARE $[CHAMPAYM]
Workers comp $[WORKPAYM]
Other $[OTHRPAYM_1]
Other $[OTHRPAYM_2]
.
.
.
Other $[OTHRPAYM_N]
Programmer:
In the summary of charges that displays above the sentence, “I show the total of all payments… as [TOTLPAYM]” distinguish different types of reserve codes, by displaying phrases “Don’t Know” or “Refused” instead of the generic word “missing.”
If there is even one reserve code entered in the SOP fields, then end the currently displayed phrase with “…although there are some payments that are missing.” For example:
“I show the total of all payments… as $30, although one or more payment is missing. Is that correct?”
“I show the total of all payments… as zero, although one or more payment is missing. Is that correct?”
Design Note #2 for C5
CHARGES
Charges: Total Amount = $[TOTLCHRG]
PAYMENTS
Patient or family $[PATPAYM]
Medicare $[CAREPAYM]
Medicaid $[AIDPAYM]
Private insurance $[PINSPAYM]
ChampVA/VA $[VAPAYM]
TRICARE $[CHAMPAYM]
Workers comp $[WORKPAYM]
Other $[OTHRPAYM_1]
Other $[OTHRPAYM_2]
.
.
.
Other $[OTHRPAYM_N]
I show the total payment of all payments received (for (MONTH)/from (BEGIN DATE) through (END DATE)) as (TOTLPAYM). Is that correct?
IF NO, CORRECT ENTRIES ABOVE AS NEEDED.
YES
NO
Programmer:
OTHRPAYM will appear on its own screen and require a selection of type (see C4h below) and dollars.
EDIT SPECS FROM WESTAT
|
DATA ITEM |
SPECIFICATIONS |
ACTION, if specification not met |
|
|
QC4 -Payment sources/amounts
CRITICAL ITEM is source of payments plus Total Payments.
The amount of Individual Payments is not a critical item.
See QC4 – QC6 Consistency notes on page 3-9. |
Must be completed if Reimbursement Type = Fee-For-Service. |
Blue Sheet, if blank. |
|
|
Every source of payment must have an amount, either $0.00 or greater than $0.00. |
Enter $0.00 for blank sources if Total Payments is given and sum of other Individual Payments equals the Total. |
||
|
Blue Sheet for blank Individual Payment if Total Payments is missing, or if sum of other sources does not equal Total. |
|||
|
DK or RF are acceptable. |
Change DK to –8. Change RF to – 7. |
||
|
If OTHER is answered, there must be an answer on the SPECIFY line. |
Blue Sheet if missing. |
||
|
If the answer is written outside of the answer line, circle the answer. |
|||
|
Answer on the SPECIFY line needs review. Sometimes the answer is written outside the line, as a comment.
|
If the answer is written outside of the Specify line, and it is on the Decision Log, circle the answer to indicate that it should be Caded. Yellow Sheet if it is not on the Decision Log. |
||
|
“HMO” is not acceptable as a SPECIFY answer. “Public” is not acceptable as a SPECIFY answer. The name of an insurance co. is not acceptable as a SPECIFY answer. Note: the same insurance company may provide private insurance and also administer Medicare and/or Medicaid payments. |
Blue sheet, asking which type of insurance. Note: the same insurance company can provide private insurance and also administer Medicare and/or Medicaid payments. |
||
|
Expect that an answer on line h OTHER/SPECIFY will have a comparable answer in QC6 line h. For example, STATE PROGRAM in QC4 will have STATE PROGRAM ADJUSTMENT in QC6. Exceptions: Provider w/o or small bal adj in QC6 will not have a comparable answer in QC4. If there is no payment in QC4 line h, there may still be an adjustment in QC6. |
Yellow Sheet if there is not a comparable answer in both questions. |
||
|
Adjustments and write-offs should not be included in payments. |
Blue Sheet if comments or answer to line (h) indicate that adjustments or write-offs have been included. |
||
|
If payment by patient is $1.00 or less, expect that the insurance type will be a public type – Medicare, Medicaid, state program, etc. |
Yellow Sheet if the insurance is not government insurance. |
||
|
If a payment is made by VA, expect that the answer to QC6 will be Eligible Veteran or an OTHER/SPECIFY answer that will reflect military service. |
Yellow Sheet. |
||
|
Comments may need review. |
Compare comments about sources to the answers given in C4. Yellow Sheet if comments don’t agree with the answer to QC4.
Yellow Sheet all comments that are not included in the answer to QC4. |
||
|
Payments by three or more insurance types need managerial review. |
Look at the payment sources in all books for a patient. Yellow Sheet, if three or more insurance types. |
||
|
Lump payments need special handling. |
See Lump payment instruction sheet, on page 24. |
||
QC5- Total Payments
CRITICAL ITEM is source of payments plus Total Payments.
|
Total Payments cannot be blank.
|
Blue Sheet, if it can’t be determined. |
||
If blank and all Individual Payments are filled in with a value or with $0.00, fill in the Total Payments. |
||||
Calculator tape should be run to verify Total if there are multiple payments. Do not use the TRC’s tape. |
Run calculator tape or review tape if run by Editing assemblers. If tape doesn’t match book, write NOT OK. If tape matches book, write OK. Initial tape. |
|||
Total Payments should equal sum of Individual Payments. |
Review calculator tape. Initial tape, compare to Total. |
|||
If there is only one payment and it doesn’t agree with Total, Blue Sheet. |
||||
If the Total Payments written by the TRC is less than sum of the Individual Payments, a correction can be made if the difference is 10% or less.
Compare the amount of the difference and the Total Payment as written by the TRC.
Note that changes can affect the answers to Box 1 and QC6. |
If the difference is 10% or less than the Total, correct the Total Payment. |
|||
Blue Sheet, if the difference is greater than 10%. |
||||
Change Box 1 to the appropriate answer. |
||||
Blue Sheet, if QC6 was skipped, but now must be answered. |
||||
If the Total Payments written by the TRC are greater than the sum of the Individual Payments, the TRC must make any corrections. |
Blue Sheet, asking if we are missing a payment or service. |
|||
DK or RF is an acceptable answer. |
Change DK to – 8; Change RF to – 7. Code PL-IV as 60, critical item missing. |
|||
Booklets with DK or RF for Procedures and Charges and Payments need special review. |
Yellow Sheet if all three fields are DK or RF. |
|||
Total Payments greater than Total Charge need managerial review. |
Yellow Sheet all overpayments. |
|||
Decision Log for QC4
[PROGRAMMER NOTE: Include all “Problems” in a drop down menu at the other specify entry and program the required “decision” behind the scenes. May require implementing instructional boxes for the DCS/abstractor. For example, if the DCS selects “vocational rehabilitation” an instruction box should pop up asking the DCS to probe for source of funding: federal, state, county, other gov’t, private, etc.]
Problem |
Decision / Categorization |
State (or Federal, or County, or City) Plan ---- Plan may be Fund, Program, Grant ------ type of plan may be given ------- REMOVE Name of State if it is present |
Code by indicating source of
funds, then type of plan if given |
Examples: |
|
Nevada State Disability (SRS) |
Code in 'Other' as State Disability |
State Breast Cancer Program |
Code in 'Other' as State Breast Cancer Program |
Maryland Indigent Program |
Code in 'Other' as State Indigent Program |
Federal Grant |
Code in 'Other' as Federal Grant |
Cook County Indigent Fund |
Code in 'Other' as County Indigent Fund |
State Program |
Code in 'Other' as State Program |
Comment indicates one of the above, but it is not indicated in QC4 (line h) |
Yellow Sheet |
Comment indicates the name of an insurance company for QC4. |
Ignore the name of an insurance company if we have the type of insurance payer. |
QC4 (line h) 'Specify' answer is name of an insurance company |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Children's Special Services |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Vocational Rehabilitation |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Welfare |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Hospital |
Yellow Sheet |
Grant |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Grant - DK who is funding it |
Code in 'Other' as GRANT - DK FUNDING |
Breast Cancer Program |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Indigent Program or Fund for Indigents |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Local |
Blue Sheet to determine who is funding it , I.e. State, County, City, Other gov't, etc |
MediCal (in California) |
Code as Medicaid (C4c) |
Employer |
Yellow Sheet |
Verbiage about car/auto accident paid or auto/car insurance paid |
Code in Other as Auto Insurance |
Military |
Blue Sheet for more specific information |
Indian Health |
Code in Other as Indian Health Service |
CHDP; CHIP |
Accept, but cross out any state or county name |
WIC |
Accept, but cross out any state or county name |
AARP (American Association of Retired Persons) |
Code as Private Insurance (QC4d) |
Prepaid Mental Health Plan - State Plan |
Code In Other as State Public Mental |
HMO |
Blue Sheet to find out Insurance Type: Medicare, Medicaid, Priv Ins., Other; Ask for source of payment. |
LUMP SUM – PENDING FURTHER RTI DISCUSSION
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
QC4 – QC5 LUMP SUM INFORMATION
The DCS supplies information needed to process the lump. This is usually in the form of a label on page 2 of the first book of a lump.
Information supplied by the DCS should include:
Book numbers that are included in the lump
Total Charge of those books
Total Payments of the lump
Sources of Payments and payment by each source
Blue Sheet, if info is missing.
Run calculator tape of charges in all books of the lump to verify Total Charge. Staple and initial tape.
Blue Sheet if calculator tape doesn’t match info written by TRC.
Total Payments are not necessary if the Individual Payments are given.
If source of payment is not given, it may be possible to determine it by QC4.
If it can’t be determined, Blue Sheet.
Repeat visits charges may be involved in the lump in books # 6 and higher.
Check for repeat visits when adding charges. Each repeat visit will have the same charge as QB5b in the booklet where the repeat visit is listed. It should be part of the Total Charge.
The Lump Payment information needs to be flagged for the Receipt Staff.
Place a Post-It note on the outer edge of the first page of the lump. Write “LUMP” and the books involved.
Place a neon-green LUMP sticker on the front cover of the case above the bottom line of the grid.
If space permits, write the name of the patient and the books in the lump on the green sticker.
QC4 – QC5 LUMP SUM INFORMATION
QC6 should be the same in all books of the lump.
Blue Sheet, if answers are given but are not consistent.
If all books are blank, Blue Sheet.
If answered in the first book of the lump, but missing from the subsequent books of the lump, transfer the answer to all books of the lump.
Box 1 should be the same in all books of the lump.
If total lump charges = total lump payments, then Box 1 should be answered 1 in all books of the lump.
If total lump charges don’t equal total lump payments, then Box 1 should be answered 2 (NO) in all books of the lump.
Answer if blank.
Correct Box 1 if wrong.
This may change the skip pattern. Review QC6, if necessary.
If lump payments = lump charges, and there is only one source of payments, the lump won’t have to go for computer calculation.
Enter the payment amount equal to the charges on the line for the payment source, and on the line for Total Payments.
If there is more than one payer, the lump will have to be processed in the usual way.
[PROGRAM BEHIND THE SCENES – SHOULD NOT APPEAR ON SCREEN. VARIABLE NAME=CPAYBOX]
BOX 1
If totChrgFlag = 1 and totPayFlag = 1 (This means no reserve codes were used for any charge and payment variables)
DO TOTAL PAYMENTS EQUAL TOTAL CHARGES?
YES, AND ALL PAID BY PATIENT OR PATIENT’S FAMILY – 1 (GO TO LSPCHECK)
YES, OTHER PAYERS - 2 (GO TO C5a)
NO, PAYMENTS < CHARGES - 3 (GO TO PLC1)
NO, PAYMENTS > CHARGES - 3 (GO TO ADJEXTRA)
IF totChrgFlag =2 AND totPayFlag =2 (This means only reserve codes were used for charge and payment variables – no values recorded) –
-GO TO PLC1 (payments less than charges discrepancy questions)
IF totChrgFlag =2 AND totPayFlag =3 (This means only reserve codes were used for charges and a mix of values and reserve codes was used for payment variables)
- GO TO PLC1 (payments less than charges discrepancy questions)
IF totChrgFlag =3 AND totPayFlag =2 (This means a mix of values and reserve codes were used for charges and only reserve codes were used for payment variables)
- GO TO PLC1 (payments less than charges discrepancy questions)
IF totChrgFlag =3 AND totPayFlag =3 (This means there is a mix of values and reserve codes for charge and payment variables)
- GO TO PLC1 (payments less than charges discrepancy questions)
IF totChrgFlag =1 AND totPayFlag =2 OR totPayFlag =3, AND TOTLPAYM < TOTLCHRG (This means, if we have all the charges, but the payments are either all reserve codes, or have at least 1 reserve code, and the total payment is less than the total charge)
- GO TO PLC1 (payments less than charges discrepancy questions)
IF totChrgFlag =1 AND totPayFlag =3, AND TOTLPAYM > TOTLCHRG (This means, if we have all the charges, and the payments have at least 1 reserve code, BUT the total payment is MORE than the total charge)
GO TO ADJEXTRA (payments more than charges discrepancy questions)
PROGRAMMER NOTES
DESCRIPTION OF PROGRAMMING REQUIRED FOR BOX 1
IF C2=C5 AND ONLY C4 OPTION WITH A RESPONSE IS ‘a’ (patient or patient’s family - PATPAYM), GO TO LSPCHECK.
IF C2=C5 AND C4 OPTIONS b, c, d, e, f, g, or h HAVE A RESPONSE, GO TO C5a.
IF C2≠C5, GO TO C6.
EDIT SPECS FROM WESTAT
-
BOX 1 – Total Payments = Total
Charges or not
1 (YES), 2 (YES) or 3 (NO) must be circled.
Compare Total Charge to Total Payments.
DK or RF is not acceptable.
Circle 3 (NO).
Blue Sheet for answer to QC6, if skipped.
If 1 (YES) or 2 (YES) is circled, there should be equal dollar values greater than $0.00.
If Total Charge and Total Payments are $0.00, DK or RF, they are not equal. QC6 must be answered.
If Total Charges and Total Payments are $0.00, Yellow Sheet for Total Charges = $0.00.
Change DK or RF to 3 (NO).
Answer QC6 as – 8 (DK).
Cannot be blank.
If blank, circle the correct answer.
Compare Total Payments to Total Charges.
Look at the Source of Payments.
Should be consistent with Total Charges, Total Payments, and Source of Payments.
If answered 1 and it should be 2 or 3, change to the correct answer.
If answered 3, and should be 1 or 2, change to the correct answer.
An answer changed to 2 will follow the skip pattern to QC5a. If that is blank, write a Blue Sheet.
The skip pattern to QC5a cannot be lost.
QC5a is flagged to record the number of times it is answered.
QC5a sends the DCS back to QC4 to look at the payments again. Changes to QC4 will NOT generate a change in Box 1.
Do NOT change the answer 2 (YES) to another answer, even if it is now no longer consistent with QC4 or QC5.
Comments may need special review.
Yellow Sheet.
FOLLOW THE SKIP PATTERN
VERIFICATION OF PAYMENT
[Page 9 – VERIFICATION OF PAYMENT (1 of 1)]
ScreeN LAYOUT
C5a. I recorded that the payment(s) you received equal YES, FINAL PAYMENTS RECORDED IN C4 AND C5 =1 EQPAYOK
the charge(s). I would like to make sure that I have NO =2
this recorded correctly. I recorded that the total
payment is [SYSTEM WILL DISPLAY TOTAL
PAYMENT FROM C5]. Does this total payment
include any other amounts such as adjustments or
discounts, or is this the final payment?
IF NECESSARY, READ BACK AMOUNT(S)
RECORDED IN C4.
PROGRAMMER NOTES
[IF EQPAYOK=1 GO TO LSPCHECK, IF EQPAYOK=2 DISPLAY HARD CHECK: “IF INCORRECT, RETURN TO C4 AND CORRECT PAYMENT ENTRIES AS NEEDED.” ]
payment(s) - If C4 has one response fill: " " ELSE fill: "s".
charge(s) - If C1a and C1b both have responses fill: "s" ELSE fill: " ".
AMOUNT(S) – If C4 has one response fill: “ “ ELSE fill: “s”.
DK/REF – WILL RECEIVE A SOFT CHECK. IF SELECT SUPPRESS WILL MOVE FORWARD TO LSPCHECK.
EDIT SPECS FROM WESTAT
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
QC5a Verification of 100% payments by Other sources.
QC5a asks the DCS to verify a 100% Total Payment when at least one source of the payment is an insurance program other than the patient.
The skip pattern of Box 1 jumps over this question, unless Box 1 is answered 2.
If QC5a is blank, and Box 1 is 2 (YES, other payer), Blue Sheet for an answer to QC5a.
If QC5a is answered, and Box 1 is answered 1 or 3, cross out the answer.
PAYMENTS LESS THAN CHARGES (new section, UNDERPAYMENT)
[Page 10 – SOURCES OF PAYMENT (1 of 1)]
PLC1. It appears that the total payments were less than the total charge. Is that because …
IF THE ONLY PAYMENT FOR THIS EVENT WAS A LUMP SUM, ANSWER “NO”.
a. There were adjustments or discounts YES=1 NO=2 DISADJ
b. You are expecting additional payment YES=1 NO=2 MOREPAY
c. This was charity care or sliding scale YES=1 NO=2 SLIDSCA2
d. This was bad debt YES=1 NO=2 BADDEB2
e. Person is an eligible veteran YES=1 NO=2 ELIGVET2
PROGRAMMER NOTE:
2020 UPDATE: If MOREPAY = 1 and BADDEB2 = 1, display a soft check after BADEB2 that reads: “YOU HAVE INDICATED EXPECTING ADDITIONAL PAYMENT AND BAD DEBT AS REASONS PAYMENTS ARE LESS THAN CHARGES. PLEASE CONFIRM WITH THE POC BY ASKING: “If the patient or other payer were to try to make a payment on this bill, would you be able to accept it?” IF YES = Expecting Additional Payment from Patient. IF NO = Bad Debt. IF POC INDICATES BOTH ARE YES, SUPPRESS AND CONTINUE.”
2016 UPDATE: Create a new Section with single form called UNDERPAYMENT to contain DISADJ, MOREPAY, SLIDSCA2, BADDEB2, and ELIGVET2 spec’d above as PLC1a-d.
ELIGVET2 – allow DK/REF
If MOREPAY=1 then show C6_additional.
If [DISADJ=1 and MOREPAY=1 ] or [DISADJ=2 and MOREPAY=2 and SLIDSCA2=2 and BADDEB2=2] then show C6_additional.
If both SLIDSCA2=1 and BADDEB2=1 with no other selection, show neither ELIGVET2 or C6_additional.
If both SLIDSCA2=1 or BADDEB2=1 with no other selection, show neither ELIGVET2 or C6_additional.
2019 UPDATE: Each PLC1 item a-e (DISADJ to ELIGVET2) appears on its own screen, along with the entire PLC1 question text. The differences among screens is only the reason payments are less than charges being asked about.
ELIGVET2: Display onscreen instruction: “DCS: IF THE POC IS CONFUSED BY THE QUESTION, ANSWER THE QUESTION ‘NO’.”
DIFFERENCE BETWEEN PAYMENTS AND CHARGES
[Page 10–DIFFERENCE BETWEEN PAYMENTS AND CHARGES (1 of 1)] SCREEN LAYOUT
Are you expecting additional payment from: IF THE ONLY PAYMENT FOR THIS EVENT WAS A LUMP SUM, ANSWER “NO”.
ADJEXTRA It appears that the total payments were more than the total charges. Is that correct?
DCS: IF THE ANSWER IS “NO” PLEASE GO BACK TO C5 (VERIFY TOTAL PAYMENTS) TO RECONFIRM CHARGES AND PAYMENTS AS NEEDED
YES=1, NO=2
|
, C6_Additional, Question Q6_additional Expecting additional payment i. Patient or Patient’s Family; YES=1, NO=2 EPAYPAT j. Medicare; YES=1, NO=2 EPAYCAR k. Medicaid; YES=1, NO=2 EPAYAID l. Private Insurance; YES=1, NO=2 EPAYPINS m. VA/ChampVA; YES=1, NO=2 EPAYVA n. Tricare; YES=1, NO=2 EPAYCHAM o. Worker’s Comp; or YES=1, NO=2 EPAYWORK p. Something else? YES=1, NO=2 EPAYOTH (IF SOMETHING ELSE: What was that?) EPAYOTOS EPAYOTOSTXT
|
PROGRAMMER NOTES
2016 UPDATE:
At least one entry among the variables on screen C6_additonal must be a “1”, DK or RF. If all entries in the series are “2” (No) then administer a hard check when the user presses “Next” at C6_Additional, “You must select at least one reason for underpayment.”
At C6_Additional
If Additional pymt expected (MOREPAY) selected as a reason at PLC1, require a selection (1,DK,RF) at C6_Additional. If all are 2, administer a hardcheck. If Sliding Scale and Bad Debt options are shown, include them in the check, otherwise, exclude them.
if ( [MOREPAY] =="1" && [EPAYPAT] =="2" && [EPAYCAR] =="2" && [EPAYAID] =="2" && [EPAYPINS] =="2" && [EPAYVA] =="2" && [EPAYCHAM] =="2"
&& [EPAYWORK] =="2" && [EPAYOTH] =="2" && ([SHOW_SLIDSCA] == "No" || [SLIDSCA] =="2") && ([SHOW_BADDEB] == "No" || [BADDEB] =="2" ) )
HardCheck("ADDITIONAL PAYMENT UNSPECIFIED: You must select at least one reason for underpayment.");
-
if ( [MOREPAY] =="1" && [EPAYPAT] =="2" && [EPAYCAR] =="2" && [EPAYAID] =="2" && [EPAYPINS] =="2" && [EPAYVA] =="2" && [EPAYCHAM] =="2" &&
[EPAYWORK] =="2" && [EPAYOTH] =="2" ) )
HardCheck("ADDITIONAL PAYMENT UNSPECIFIED: You must select at least one reason for underpayment.");
if ( [MOREPAY] =="1" && [EPAYPAT] =="2" && [EPAYCAR] =="2" && [EPAYAID] =="2" && [EPAYPINS] =="2" && [EPAYVA] =="2" && [EPAYCHAM] =="2" &&
[EPAYWORK] =="2" && [EPAYOTH] =="2" ) )
HardCheck("ADDITIONAL PAYMENT UNSPECIFIED: You must select at least one reason for underpayment.");
if ( [ELIGVET2] =="2" && [EPAYPAT] =="2" && [EPAYCAR] =="2" && [EPAYAID] =="2" && [EPAYPINS] =="2" && [EPAYVA] =="2" && [EPAYCHAM] =="2" &&
[EPAYWORK] =="2" && [EPAYOTH] =="2" ) )
HardCheck("PAYMENT UNSPECIFIED: You must select at least one reason for underpayment.");
C6 - (MONTH/BEGIN DATE)
IF R_HOWBILL=1, MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL= (2 or 3) BEGIN DATE should fill with R_EVNTBEG_D from E1
After C6 - [GO TO LSPCHECK]
(less than/more than) - If C5 < C2 fill: "less than", else if C5 > C2 fill: "more than".
DK/REF – GO TO LSPCHECK
C6p should each be set up as a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the question that reads: Any more expected payments? YES=1 NO=2
(3) The “something else” option should be set up so a response can be selected from a list, or entered in as text.
C6p - The EPAYOTOSTXT variable was added to record free-form text for the “Other, Specify” options. Interviewers will be able to record responses in the text box that do not occur in the listed options. DCS instruction onscreen for EPAYOTOSTXT reads “EXPECTING OTHER ADDITIONAL PAYMENT…”, “PLEASE SPECIFY OTHER.” EPAYOTOSTXT field allows up to 50 characters.
C6p – Include the following options in listed options for the “Other Specify”:
Auto or Accident Insurance
Indian Health Service
State Public Mental Plan
State/County/Local program
Other
ALSO ALLOW SYSTEM TO PULL UP NAME OF SOURCE SPECIFIED IN C4h.
2019 UPDATE: Each C6_additional item i-p (EPAYPAT to EPAYOTH) appears on its own screen, along with the entire C6_additional question text. The differences among screens is only the source of additional expected payment being asked about.
2019 UDPATE: IF PLC1 ITEMS DISADJ, MOREPAY, SLIDSCA2, BADDEB2, AND ELIGVET2 ALL = 2, AND C6_ADDITIONAL ITEMS EPAYPAT, EPAYCAR, EPAYAID, EPAYPINS, EPAYVA, EPAYCHAM, EPAYWORK, AND EPAYOTH ALL =2, DISPLAY HARDCHECK: “YOU MUST SELECT AT LEAST ONE REASON PAYMENTS ARE LESS THAN CHARGES. RETURN TO PLC1 ITEMS AND/OR C6_ADDITIONAL ITEMS AND SELECT THE REASON(S).”
2019 UPDATE: IF ADJEXTRA = 2, DISPLAY A HARD CHECK: “IF THE ANSWER IS ‘NO,’ PLEASE GO BACK TO C5 (VERIFY TOTAL PAYMENTS) TO RECONFIRM CHARGES AND PAYMENTS AS NEEDED.”
EDIT SPECS FROM WESTAT
DATA ITEM |
SPECIFICATIONS |
ACTION, if specification not met |
QC6 a – r Reason for PAYMENTS LESS THAN CHARGES
See QC4-QC6 CONSISTENCY notes below.
|
If payments are less than charges, there must be a YES (1) answer on lines a – r. |
Blue Sheet, if there is no YES answer, and payments are less than charges. |
The answer must be consistent with the source of payments on QC4. |
Check the answer with the QC4 – QC6 CONSISTENCY reference sheet below labeled “QC4 and QC6 Consistency Notes”. |
|
YES (1) or NO (2) must be circled for each choice. Since YES (1) may be answered for more than one choice, only the TRC can answer NO (2). |
Blue Sheet if missing for any choice. Blue Sheet if both YES (1) and NO (2) are circled for a choice. |
|
Since more than one answer can be YES, only the TRC can write NO for an answer if payments are less than charges. |
Blue Sheet if only YES answer is circled, and NO answers are blank, and the payments are less than charges. Let the TRC fill in the NO answers. |
|
If there is a YES answer in PAYMENTS MORE THAN CHARGES section, all choices in the PAYMENTS LESS THAN CHARGES SECTION should be NO (2). |
Blue Sheet if there is a YES answer in both PAYMENTS LESS and PAYMENTS MORE sections. |
|
Circle NO (2) for all answers in the PAYMENTS LESS section, if all answers are blank and there is a YES (1) answer in the PAYMENTS MORE section. |
||
If OTHER is answered, there must be an answer on the SPECIFY line (QC6 line h or line p). Sometimes the answer is written outside the line, as a comment.
Answer on the SPECIFY line (QC6 line h or line p) needs review. |
Check Decision log for all Specify answers. If it is on the Decision log, follow directions given there. If the answer is not there, Yellow Sheet. |
|
Blue Sheet if Specify answer is missing. |
||
If the answer is written outside of the Specify line, circle the answer if it is on the Decision Log to indicate that it should be Caded. Yellow Sheet if it is not on the Decision Log. |
||
DATA ITEM QC6 a – r Reason for PAYMENTS LESS THAN CHARGES
See QC4-QC6 CONSISTENCY notes QC6 a – r Reason for PAYMENTS LESS THAN CHARGES
See QC4-QC6 CONSISTENCY notes
|
QC6 line h answers should also be reflected in QC4 unless total pay was $0.00. State program paid; State program adj. Exceptions: Provider w/o or sm ball adj |
Yellow Sheet. |
Provider write-off and Small balance write-off are acceptable answers on line h. |
Accept. |
|
Courtesy Discount (line d) may need review. |
If the only payer is an insurance, Yellow Sheet. |
|
If there are three insurance types, managerial review is needed. |
If the sources of payment include three or more insurance types, Yellow Sheet. This may be indicated by the answers to QC4 and QC6 in all books for a patient. |
|
Adjustments are acceptable with no payment from that source in QC4. |
Accept, unless it looks like wrong answer was circled. For example, QC4 says Medicare paid $0.00; QC6 says Medicare adjustment or limit. |
|
Comments may need review. |
Check the Decision Log. Follow instructions. It may be permissible to move the comment to QC6 (line h or p). |
|
If Comments say “in collections” expect that the answer to QC6 will be Expecting Patient Payment or Bad Debt. |
Accept if QC6 is answered “Expecting Payment from Patient” and/or “Bad Debt.” Otherwise, Yellow Sheet. |
|
“In collections” cannot be an answer on the Specify line. If “Expecting Payment from Patient” and/or “Bad Debt” answers are given, cross out “in collections” and change line p to 2 (NO). If these are not answered, Yellow Sheet. |
||
Books should be compared for consistency. |
Review all books for a patient. It is not necessary for books to be identical, but if it looks like the wrong answer was given in a book, Blue Sheet. |
|
There should not be an adjustment in the expecting payments section (line p). |
Blue Sheet if the answer to this question is not a payer source. |
|
QC6 s – v Reason for PAYMENTS MORE THAN CHARGES
See QC4-QC6 CONSISTENCY notes
|
OVERPAYMENTS NEED REVIEW |
Yellow Sheet. |
If payments are more than charges, there must be a YES (1) answer on lines s-v |
Blue Sheet. |
|
More than one YES answer is acceptable. |
Blue Sheet if the NO answers are missing and payment is more than charges. |
|
The answer must be consistent with the source of payments on QC4. |
Check the answer with the QC4 – QC6 CONSISTENCY notes on page 3-9, or on page 4-28. |
|
YES (1) or NO (2) must be circled for each choice. Since YES (1) may be answered for more than one choice, only the TRC can answer NO (2). |
Blue Sheet if missing and payment is less than charge. |
|
Blue Sheet if only YES answer is circled, and the NO answers are blank, if payments are more than charges. Let the TRC fill in the NO answers. |
||
If there is a YES answer in PAYMENTS LESS THAN CHARGES section, all choices in the PAYMENTS MORE THAN CHARGES SECTION should be NO (2).
Review the payments and charges. Are payments less or more than charges? |
Blue Sheet if there is a YES answer in both PAYMENTS LESS and PAYMENTS MORE sections. |
|
If Payments are Less than Charges, and answers in the PAYMENTS MORE section are all blank, and there is a YES (1) answer in the PAYMENTS LESS section,. Circle NO (2) for all answers in the PAYMENTS MORE section. |
||
If OTHER is answered, there must be an answer on the SPECIFY line (QC6 line v). Sometimes the answer is written outside the line, as a comment.
Answer on the SPECIFY line (QC6 line v) needs review. |
Check Decision log for all Specify answers. If it is on the Decision log, follow directions given there. If the answer is not there, Yellow Sheet. |
|
Blue Sheet if Specify answer is missing. |
||
If the answer is written outside of the Specify line, and it is on the Decision Log, circle the answer to indicate that it should be Caded. Yellow Sheet if it is not on the Decision Log. |
||
If there are three insurance types, review is needed. |
If the sources of payment include three or more insurance types, Yellow Sheet. This may be indicated by the answers to QC4 and QC6 in all books, looked at together. |
|
OTHER/SPECIFY answers in QC6 line v should be reflected in an OTHER/SPECIFY answer in QC4. State program paid; State program adj |
Yellow Sheet.
|
QC4 AND QC6 CONSISTENCY NOTES
PAYER IN QC4 |
ANSWER TO QC6 |
Medicare |
Accept any of these alone: Medicare Adjustment, Contractual Arrangement, Expecting Payment from any source, Charity, or Bad Debt. Accept Medicare Adjustment plus any of the following: Medicaid Adjustment, Contractual Arrangement, Courtesy Discount, Expecting Payment from any source, Charity or Bad Debt. If Insurance Write-Off is answered, Yellow Sheet. If the only answer is an adjustment or limit or arrangement other than Medicare, look for an indication* that this other source is involved. If no indication, Blue Sheet. |
Medicaid |
Accept any of these alone: Medicaid Adjustment; Expecting Payment from any source, Charity, or Bad Debt.
Accept Medicaid Adjustment plus any of the following: Medicare Adjustment, Contractual Arrangement, Courtesy Discount, Expecting Payment from any source, Charity or Bad Debt.
If Insurance Write-Off is answered, Yellow Sheet.
If the only answer is any adjustment or limit or arrangement other than Medicaid, look for an indication* that the other source is involved. If no indication, Blue Sheet. |
Private Insurance |
Accept any of these alone: Contractual Arrangement; Expecting Payment from any source, Charity, or Bad Debt.
Accept Contractual Arrangement plus any of the following: Medicare Adjustment, Medicaid Adjustment, insurance w/o, Courtesy Discount, Expecting from any source, Charity or Bad Debt.
If only answer is any adjustment or limit other than Private Insurance, look for indication* that the other source is involved. If no indication, Blue Sheet. |
TRICARE, Champus, ChampVA |
Accept anything that is acceptable for Private Insurance, and/or accept Eligible Veteran or OTHER/SPECIFY: Tricare Adjustment or Champus Adjustment.
May be the primary insurance or secondary to other kinds of insurance. |
VA or Indian Health |
Usually says “ELIGIBLE VETERAN” or OTHER/SPECIFY: “ELIGIBLE…” There may be no payment or payment by any source.
If there is a payment by another source, QC6 may refer to that source, either alone or in addition to Eligible Veteran (or Other/Specify “Eligible…” answer.
If Insurance Write-Off is answered, Yellow Sheet.
Accept Courtesy Discount, Charity and Bad Debt in addition to “Eligible…” or other insurance adjustment. |
Workers’ Comp
|
Should say “Workers’ Comp Adjustment.” If missing, Blue Sheet.
Accept Courtesy Discount, Charity and Bad Debt in addition to Workers’ Comp Adjustment.
If Insurance Write-Off is answered, Yellow Sheet.
Expect that no other insurance will be involved. If Workers’ Comp is given with any other insurance, Yellow Sheet. |
*Look for INDICATIONS OF ADDITIONAL SOURCES OF PAYMENT in:
QC4 (payers) in other books
Comments
Expecting Payment section
Additional instruction copied and pasted from Westat’s hardcopy edit manual for OB.
DECISION LOG FOR QC6
[PROGRAMMER NOTE: Include all “Problems” in a drop down menu at the other specify entry and program the required “decision” behind the scenes. May require implementing instructional boxes for the DCS/abstractor. For example, if the DCS selects “insurance was never billed” an instruction box should pop up asking the DCS to probe to include type of insurance if know, such as MEDICARE NEVER BILLED]
Problem |
Decision / Categorization |
Payment Less than Charges |
If instructions say to add
an answer to line h or line p, change the YES/NO answer to 1 and
cross out the answer 2. |
Underpayment exists in Q(C4) by a State (or Federal, or County, or City) Plan ---- Plan may be Fund, Program, Grant ------ type of plan may be given ------- REMOVE Name of State if it is present |
Code in 'OTHER' as (name of source given in Q(C4h)). |
Examples: |
|
Nevada State Disability |
State Disability. |
State Breast Cancer Program |
State Breast Cancer Program. |
Maryland Indigent Program |
State Indigent Program. |
Federal Grant |
Federal Grant. |
Cook County Indigent Fund |
County Indigent Fund. |
State Program |
State Program. |
Zero total payment in Q(C4) but comment about a State (or Federal, or County, or City) Plan ---- Plan may be Fund, Program, Grant ------ type of plan may be given ------- REMOVE Name of State if it is present |
If TRC says Charity care,
accept as is. |
Comment says that insurance was never billed |
Code in 'Other' (line h) as
NEVER BILLED. |
Comment says Insurance denied payment. |
Code in 'Other' (line h) as
INSURANCE DENIED. |
Comment mentions billing error. |
Code in 'Other' (line h) as
Billing Error. |
Comment mentions untimely filing, billed late. |
Code in 'Other' (line h) as
Billed Late. |
Comment mentions Insurance denied, with an amount, such as Private Insurance denied $52.50. |
Code in 'Other' (line h) as
INSURANCE DENIED. |
Comment mentions that the insurance doesn't cover a procedure. |
Code in 'Other' (line h) as
INSURANCE DENIED: PROCEDURE NOT COVERED. |
Comment mentions that insurance doesn't cover if no pre-authorization |
Code in 'Other' (line h) as
INSURANCE DENIED: NO PRE-AUTHORIZATION. |
Comment mentions nurse visit not covered |
Code in 'Other' (line h) as
INSURANCE DENIED: NURSE VISIT. |
Comment says patient paid the deductible. |
Do not code in 'Other' (line
h). |
Comment says insurance made an adjustment. |
Do not code in 'Other' (line
h). |
Comment mentions Collection Agency or " in Collections" |
Do not code in 'Other' line
h or line p. |
Collection Agency or "in collections" is Other/Specify answer (line h or line p) |
Cross out "in
collections," etc. as the 'Specify' answer (line h or line
p). |
Small balance w/o (Small balance write off) |
Code in Other as Small Balance W/O |
Small balance Adj (Small balance adjustment) |
Code in Other as Small balance Adj |
Military |
Blue Sheet for more specific information |
Dependent of active duty military / Active duty military dependent |
Code in 'other' as Eligible Active Duty Fam Mem |
Active duty armed forces member / Active duty military |
Code in 'Other' as Eligible Active Duty |
Active duty family member |
Code in 'Other' as Eligible Act Duty Fam Mem |
Retired veteran / Retired military |
Code in 'Other' as Eligible Retiree |
Retired veteran's family member |
Code in 'Other' as Eligible Retiree Fam Mem |
Retired Military Dependent |
Code in 'Other' as Eligible Retiree Fam Mem |
Veteran's family member |
Code in 'Other' as Eligible Veteran Fam Mem |
Indian Health |
Code in 'Other' as Eligible Native American |
Clerical fee; administrative fee |
YELLOW SHEET |
Grant - DK who is funding it |
Code in 'Other' as Grant - DK who is funding it. |
HMO |
Blue Sheet for type of insurance: Medicare, Medicaid, or Private, other |
Comments say No payments due to Federal Vaccines given/ Fed gov't supplied vaccines |
Code in 'Other' (line h) as Federal Vaccine Program. |
Payment More than Charges |
Yellow Sheet ALL OVERPAYMENTS |
Tricare (or Champus) payment exceeds charges |
Accept Private Insurance adjustment or, in 'OTHER', as Tricare (or Champus) Adjustment |
Overpayment exists in Q(C4) by a State (or Federal, or County, or City) Plan ---- Plan may be Fund, Program, Grant ------ type of plan may be given ------- REMOVE Name of State if it is present |
Code in 'OTHER' as (name of source given in Q(C4h)). |
Examples: |
|
Nevada State Disability |
Code in 'Other' (line v) as State Disability. |
State Breast Cancer Program |
Code in 'Other' as State Breast Cancer Program. |
Maryland State Indigent Program |
Code in 'Other' as State Indigent Program. |
Federal Grant |
Code in 'Other' as Federal Grant. |
Cook County Indigent Fund |
Code in 'Other' as County Indigent Fund. |
State Program |
Code in 'Other' as State Program. |
Comment mentions Patient Credit, Patient Overpayment; Patient has a balance |
Yellow Sheet. |
LUMP SUM PAYMENTS
LSPCHECK
WAS THIS EVENT COVERED BY A LUMP SUM?
1 YES
2 NO
PROGRAMMING NOTE:
IF (all source of payment fields PATPAYM to WORKPAYM and OTHRPAYM have entries of 0.00) or (TOTLPAYM is 0.00 or missing)
AND a-e = NO ( DISADJ, MOREPAY, SLIDSCA2, BADDEB2, ELIGVET2) AND i-p = NO (EPAYPAT, EPAYCAR, EPAYIAD, EPAYPINS, EPAYVA, EPAYCHAM, EPAYWORK, EPAYOTH ) AND (LSPCHECK=”No”) display a hard error at LSPCHECK, “PAYMENT VALIDATION FAILED: No payment source or reason(s) identified. Return to Sources of Payment or Payments NE Charges, or record Lump Sum Payment here.” This hard error will require user to correct one of those conditions or break off the event form
DK/REF ALLOWABLE and SKIP TO END OF EVENT FORM
CAPITATED BASIS
NOTE: See end of section for edit specs from Westat for questions C7a, C7b, C7c, C7d, C7e, and C7f.
[Page 11–CAPITATED BASIS (1 of 4)] |
|
SCREEN LAYOUT C7a. What kind of insurance plan covered the patient (for (MONTH)/from (BEGIN DATE) through (END DATE))? Was it:
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
OTHER SPECIFY: PROBE FOR SOURCE OF FUNDS AND TYPE OF PLAN.
C7b. Was there a co-payment for any of the services provided (for (MONTH)/from (BEGIN DATE) through (END DATE))?
|
a. Medicare; YES=1, NO=2 COVCARE b. Medicaid; YES=1, NO=2 COVAID c. Private Insurance; YES=1, NO=2 COVPINS d. VA/ChampVA; YES=1, NO=2 COVVA e. Tricare; YES=1, NO=2 COVCHAM f. Worker’s Comp; or YES=1, NO=2 COVWORK g. Something else? YES=1, NO=2 COVOTHR (IF SOMETHING ELSE: What was that?) COVOTOS COVOTOSTXT
YES=1, NO=2 ANYCOPAY
|
PROGRAMMER NOTES
This screen will require special layout as mentioned in NOTE 5 on pg. 5 of this document. This is due to question looping and interviewer instructions/definitions.
C7a & C7b - (during (MONTH)/from (BEGIN DATE) through (END DATE))
IF R_HOWBILL=1, fill “during (MONTH)”
MONTH should fill with EVNTBEGM, EVNTBEGY from E1
IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)”
BEGIN DATE should fill with R_EVNTBEG_D from E1
END DATE should fill with R_R_EVNTEND_D from E1
C7a(g) - The COVOTOSTXT variable was added to record free-form text for the “Other, Specify” option. Interviewers will be able to record responses in the text box that do not occur in the listed options.Field allows up to 50 characters. Screen reads: “OTHER INSURANCE PLAN…” “PLEASE SPECIFY OTHER”
C7a(g) is a question loop that will require:
(1) A HISTORY BOX to display responses already collected.
(2) A question to appear after each iteration of the question that reads:
Any more plans? YES=1 NO=2
(3) The “something else” option should be set up so a response can be selected from listed options, or entered in as text.
C7a(g) – Include the following options in listed options for the “Other Specify”;
Auto or Accident Insurance
Indian Health Service
State Public Mental Plan
State/County/Local program
Other
C7b - [IF ANYCOPAY=2 GO TO C7e]
C7a - DK/REF– CONTINUE TO C7b
C7b - DK/REF– GO TO C7e
2021 UPDATE: IF C7a a-g (COVCARE, COVAID, COVPINS, COVVA, COVCHAM, COVWORK, COVOTHR) all equal 2 (NO), display soft check:
YOU HAVE INDICATED CAPITATED PAYMENT, BUT ENTERED ‘NO’ FOR ALL INSURANCE TYPES. PLEASE CHECK THE RECORDS AGAIN AND/OR PROBE WITH THE POC TO DETERMINE THE INSURANCE PLAN(S) TYPE THAT COVERED THIS EVENT, AND CHANGE THE ANSWER FOR THAT ITEM. OR CLICK ‘SUPPRESS’ TO CONTINUE.
2019 UPDATE: Each C7a item a-g (COVCARE to COVOTHR) appears on its own screen, along with the entire C7a question text. The differences among screens is only the payer type (Medicare, Medicaid, etc.).
[Page 12–CAPITATED BASIS (2 of 4)] SCREEN LAYOUT C7c. What was the total of all co-payments (during (MONTH) /from(BEGIN DATE) through (END DATE))?
C7d. Who paid the co-payment? Was it:
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
PROGRAMMER NOTES C7d - This screen will require special layout due to question looping and interviewer instructions/definitions.
C7c - DOLLAR AMOUNTS SHOULD BE FORMATTED TO INCLUDE COMMAS and DECIMAL POINTS
C7c - (for (MONTH)/from (BEGIN DATE) through (END DATE)) IF R_HOWBILL=1, fill “during (MONTH)” MONTH should fill with EVNTBEGM, EVNTBEGY from E1 IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)” BEGIN DATE should fill with R_EVNTBEG_D from E1 END DATE should fill with R_EVNTEND_D from E1
C7d(e) - The CPAYOTOSTXT variable was added to record free-form text for the “Other, Specify” option. Interviewers will be able to record responses in the text box that do not occur in the listed items.
C7d(e) is a question loop that will require: (1) A HISTORY BOX to display responses already collected. (2) A question to appear after each iteration of the question that reads: Any more payers? YES=1 NO=2 (3) The “something else” option should be set up so a response can be selected from listed items, or entered in as text.
C7d(e) – Include the following listed options for the “Other Specify”; Auto or Accident Insurance Indian Health Service State Public Mental Plan State/County/Local program Other
C7d(e) OCPAYOTOSTXT item screen text: “OTHER SOURCE OF CO-PAYMENT…” “PLEASE SPECIFY OTHER”. Text field allows up to 50 characters.
C7c - DK/REF – CONTINUE TO C7d C7d - DK/REF – CONTINUE TO C7e
2019 UPDATE: Each C7d item a-e (CPAYPAT to CPAYOTHR) appears on its own screen, along with the entire C7d question text. The differences among screens is only the payer type (Patient or Patient’s Family, Medicare, Medicaid, etc.).
[Page 13–CAPITATED BASIS (3 of 4)] SCREEN LAYOUT C7e. Do your records show any other payments for any of the services provided (during (MONTH)/from (BEGIN DATE) through (END DATE))? PROGRAMMER NOTES C7e - (during (MONTH)/from (BEGIN DATE) through (END DATE)) IF R_HOWBILL=1, fill “during (MONTH)” MONTH should fill with EVNTBEGM, EVNTBEGY from E1 IF R_HOWBILL=(2 or 3), fill “from (BEGIN DATE) through (END DATE)” BEGIN DATE should fill with R_EVNTBEG_D from E1 END DATE should fill with R_R_EVNTEND_D from E1
DK/REF – GO TO EXIT
[IF OTHPAY=2 GO TO EXIT]
|
$ COPAYAMT
a. Patient or Patient’s Family; YES=1, NO=2 CPAYPAT b. Medicare; YES=1, NO=2 CPAYCARE c. Medicaid; YES=1, NO=2 CPAYAID d. Private Insurance; or YES=1, NO=2 CPAYPINS e. Something else? YES=1, NO=2 CPAYOTHR (IF SOMETHING ELSE: What was that?) CPAYOTOS OCPAYOTOSTXT
|
YES=1, NO=2 OTHPAY
|
[Page 14–CAPITATED BASIS (4 of 4)] SCREEN LAYOUT C7f. From which of the following other sources has your organization received payment and how much was paid by each source? Please include all payments that have taken place between (MONTH/BEGIN DATE) and now for this care. Was it:
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
RECORD PAYMENTS FROM APPLICABLE PAYERS
Any more sources?
PROGRAMMER NOTES C7f: Each of the fields requires a non-blank entry, as was done for sources of payment. Entries of 0, DK, RF are allowed here.
This screen will require special layout due to question looping and interviewer instructions/definitions.
2019 UPDATE: Each C7f item a-h (OTHPAT to OTHOTHR) appears on its own screen, along with the entire C7f question text. The differences among screens is only the payer type (Patient or Patient’s Family, Medicare, Medicaid, etc.).
C7f - (MONTH/BEGIN DATE) IF R_HOWBILL=1, MONTH should fill with EVNTBEGM, EVNTBEGY from E1 IF R_HOWBILL= (2 or 3) BEGIN DATE should fill with R_EVNTBEG_D from E1
(h) is a question loop that will require: (1) A HISTORY BOX to display responses already collected. (2) A question to appear after each iteration of the question that reads: Any more sources? YES=1 NO=2 (3) The “something else” option should be set up so a response can be selected from listed options, or entered in as text.
C7f(h) - The OTHOTOSTXT variable was added to record free-form text for the “Other, Specify” option. Interviewers will be able to record responses in the text box that do not occur in the listed options.
(h) – Include the following options in listed options for the “Other Specify”; Auto or Accident Insurance Indian Health Service State Public Mental Plan State/County/Local program Other
C7f(h) OTHOTOSTXT screen text: “OTHER PAYMENT SOURCE…” “PLEASE SPECIFY OTHER”.
OTHOTOSTXT field allows up to 50 characters.
DOLLAR AMOUNTS SHOULD BE FORMATTED TO INCLUDE COMMAS and DECIMAL POINTS DK/REF – CONTINUE TO EXIT
|
SOURCE a. Patient or Patient’s Family; b. Medicare; c. Medicaid; d. Private Insurance; e. VA/ChampVA; f. Tricare; g. Worker’s Comp; or h. SOMETHING ELSE? (IF SOMETHING ELSE: What was that?) OTHOTOS OTHOTOSTXT |
PAYMENT AMOUNT $OTHPAT $OTHCARE $OTHAID $OTHPINS $OTHVA $OTHCHAM $OTHWORK
$OTHOTHR
|
EDIT SPECS FROM WESTAT
DATA ITEM |
SPECIFICATIONS |
ACTION, if specification not met |
|
Capitated Section
Completed if QC3 is Capitated (2). |
Entire Capitated Section cannot be DK or RF. |
Blue Sheet, to verify that Reimbursement type is Capitated. |
|
DK or RF is acceptable for individual answers in the Capitated Section, as long as entire section is not DK or RF. |
Accept DK or RF. Change to -7 or -8. Yellow Sheet, if questionable. |
||
QC7a – Capitated – what kind of insurance |
Must be completed if Reimbursement Type in QC3 = Capitated Basis |
Blue Sheet, if no answers are YES (1). |
|
More than one answer of YES is acceptable. |
Blue Sheet, if the NO (2) answers are not circled, and there is a YES (1) answer. |
||
Answers should agree in all books for a pair. |
Yellow Sheet, if answers differ in books for a pair. |
||
If SOMETHING ELSE is answered, there must be an answer on the SPECIFY line. |
Blue Sheet if missing. |
||
Answer on the SPECIFY line needs review. |
Check Decision log. If it is on the Decision log, follow directions given there. If the answer is not there, Yellow Sheet. |
||
“HMO,” “Public,” or the name of an insurance company is not acceptable as a SPECIFY answer. |
Blue sheet, asking which type of insurance. Note: the same insurance company can provide private insurance and also administer Medicare and/or Medicaid payments. |
||
If “HMO, DK type” Yellow Sheet. |
|||
QC7b – Any Co-pay |
1 or 2 circled must be circled. |
If blank and there is no indication of a co-payment, circle NO (2). |
|
QC7c - Co-payment amount |
If QC7b is YES, there must be an amount. |
Blue Sheet. |
|
Co-pay range is typically > 0 and <=$50. |
Yellow Sheet. |
||
Co-pay amount is typically a whole dollar number. |
Yellow Sheet. |
||
DK or RF is acceptable.
|
Change DK to – 8. Change RF to – 7. |
||
If payment by patient is $1.00 or less, expect that the insurance type will be a public type – Medicare, Medicaid, state program, etc. |
Yellow Sheet if there is another insurance type indicated. |
||
QC7d - Co-payment payer |
If QC7b is YES, there must be a co-payer source. |
Blue Sheet. |
|
Sources other than patient or patient’s family need review. |
Yellow Sheet if source of co-pay is not patient or patient’s family. |
||
Answers of more than one source need review. |
Yellow Sheet. |
||
Answer on the SPECIFY line needs review. |
Check Decision log. If it is on the Decision log, follow directions given there. If the answer is not there, Yellow Sheet. |
||
“HMO,” “Public,” or the name of an insurance company is not acceptable as a SPECIFY answer. |
Blue Sheet, asking which type of insurance. Note: the same insurance company can provide private insurance and also administer Medicare and/or Medicaid payments. |
||
QC7e Capitated Secondary Payment? |
Must be answered 1 (YES) or 2 (NO). |
If blank and nothing indicates that there is a Capitated Secondary payment, Circle 2 (NO). |
|
Capitated Secondary Payments need review. |
Yellow Sheet if YES. |
||
QC7f – Source(s) and amount of payment for CAPITATED SECONDARY PAYMENT |
If QC7e is YES (1), a payment amount must be filled in for at least one source. |
Blue Sheet, if there is no amount given. |
|
If there is an amount, the Capitated Secondary Payment needs special review. |
Yellow Sheet all Capitated Secondary Payments. |
||
DK or RF is acceptable. |
Change DK to –8 and RF to –7; Yellow Sheet as a Capitated Secondary Payment. |
||
If question is not skipped (QC7e is YES), all sources of payment must have a dollar value. |
If there is a dollar amount for one source, fill in $0.00 for all the other sources. Do not leave any lines blank, unless the question is skipped (when QC7e is NO). |
||
Answer on the SPECIFY line (h) needs review. |
Check Decision log. If it is on the Decision log, follow directions given there. If the answer is not there, Yellow Sheet. |
||
“HMO,” “Public,” or the name of an insurance company is not acceptable as a SPECIFY answer. |
Blue Sheet, asking which type of insurance. Note: the same insurance company can provide private insurance and also administer Medicare and/or Medicaid payments. |
||
Note: There is no Total Payments field for this question. |
If the TRC has written the Total Secondary Capitated Payment on the last line (for Other/Specify payment), cross it out. |
||
Decision Log for C7a, C7d, and C7f (same as Decision Log for QC4)
[PROGRAMMER NOTE: Include all “Problems” in a drop down menu at the other specify entry and program the required “decision” behind the scenes. May require implementing instructional boxes for the DCS/abstractor. For example, if the DCS selects “vocational rehabilitation” an instruction box should pop up asking the DCS to probe for source of funding: federal, state, county, other gov’t, private, etc.]
Problem |
Decision / Categorization |
State (or Federal, or County, or City) Plan ---- Plan may be Fund, Program, Grant ------ type of plan may be given ------- REMOVE Name of State if it is present |
Code by indicating source of
funds, then type of plan if given |
Examples: |
|
Nevada State Disability (SRS) |
Code in 'Other' as State Disability |
State Breast Cancer Program |
Code in 'Other' as State Breast Cancer Program |
Maryland Indigent Program |
Code in 'Other' as State Indigent Program |
Federal Grant |
Code in 'Other' as Federal Grant |
Cook County Indigent Fund |
Code in 'Other' as County Indigent Fund |
State Program |
Code in 'Other' as State Program |
Comment indicates one of the above, but it is not indicated in C7a (line g)/C7f (line h) |
Yellow Sheet |
Comment indicates the name of an insurance company for C7a/C7f. |
Ignore the name of an insurance company if we have the type of insurance payer. |
C7a (line g)/C7f (line h) 'Specify' answer is name of an insurance company |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Children's Special Services |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Vocational Rehabilitation |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Welfare |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Hospital |
Yellow Sheet |
Grant |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Grant - DK who is funding it |
Code in 'Other' as GRANT - DK FUNDING |
Breast Cancer Program |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Indigent Program or Fund for Indigents |
Blue Sheet to determine source of funding: Federal, State, County, Other gov't, Private etc |
Local |
Blue Sheet to determine who is funding it , I.e. State, County, City, Other gov't, etc |
MediCal (in California) |
Code as Medicaid (C7a (line b)/C7f (line c)) |
Employer |
Yellow Sheet |
Verbiage about car/auto accident paid or auto/car insurance paid |
Code in Other as Auto Insurance |
Military |
Blue Sheet for more specific information |
Indian Health |
Code in Other as Indian Health Service |
CHDP; CHIP |
Accept, but cross out any state or county name |
WIC |
Accept, but cross out any state or county name |
AARP (American Association of Retired Persons) |
Code as Private Insurance (C7a (line c)/C7f (line d)) |
Prepaid Mental Health Plan - State Plan |
Code In Other as State Public Mental |
HMO |
Blue Sheet to find out Insurance Type: Medicare, Medicaid, Priv Ins., Other; Ask for source of payment. |
EDIT SPECS FROM WESTAT
Home Care Booklet, Page 7
-
DATA ITEM
SPECIFICATIONS
ACTION, if specification not met
E5 – All months covered?
1 or 2 must be circled.
Blue Sheet, unless there are exceptions, as indicated below.
If this is NOT the last book, 2 (NO, need to cover additional events) should be circled.
If NOT the last book, change blank to 2 (NO). If NOT the last book, change 1 to 2 (NO).
If the last book will be deleted because it is for a month in 2022, the answer in that book can be transferred to the last book in 2022.
Transfer answer from 2022 book, making a notation that this is “per Jan (or Feb) 2022 book.”
There cannot be more than twelve books.
If 2 (NO) is circled, and this is the last book, Blue Sheet.
Exception: If there is a book for all 12 months, Circle 1 (YES) in the December book.
If blank in the last book, review QE6.
If QE6 is blank, Blue Sheet for QE5.
If QE6 is answered, answer YES in QE5, because the TRC has indicated that this is the last book by answering QE6.
E6 – In last book, did we get as many months are we expected?
If not, why not?
This question is only answered in the last book for a patient.
If not last book, but this question is answered, cross out.
If last book, QE6 cannot be blank.
Review the total number of events collected from the provider.
Compare the total events collected with the total events expected on the Patient Data Form.
Determine answer to QE6 and circle appropriate response.
If 1 is circled,
The provider gave us the same number of Months of service that the patient gave us, or the provider gave us more than the patient gave us.
Compare months collected to total months on Patient Data Form.
Blue Sheet, if we didn’t get as many events as we expected.
If 2 is circled,
The provider gave us less months of service than the patient reported. An explanation must be recorded by the TRC.
Blue Sheet, if events are missing and no explanation given.
If 2 is circled, but a review of the PDF shows that we have collected enough events, change answer to 1, unless it looks like a month is missing. Yellow Sheet, if the explanation looks like a month was not collected.
ALL EXPLANATIONS NEED MANAGERIAL REVIEW.
Yellow Sheet, if events are missing and explanation is given.
If events are not missing, but an explanation is given, cross out explanation, unless the explanation looks like a month was not collected. Yellow Sheet for possible missing months.
FINISH SCREEN
ENTER 1 TO FINALIZE CASE.
PROGRAMMER NOTES
At this screen, users will enter a 1 and Enter to finalize the event form.
OP2-11_HCH_EF_v1.0
Page
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | MEDICAL EVENT FORM |
| Author | Doris R. Northrup |
| File Modified | 0000-00-00 |
| File Created | 2024-07-21 |
© 2025 OMB.report | Privacy Policy