Description
|
Interviewer-administered form
|
Self-administered web form
|
INTRODUCTION
Allow respondent to provide information on behalf of their
spouse or child
|
Hello, my name is <interviewer name>. I am from
<interviewer health department name>. We are
contacting you because you (or the ill person) were recently sick
with a Shigella infection, also called
shigellosis. Shigella are a group of bacteria
that cause diarrheal illness. We are trying to determine how you
(or the ill person) became sick with a Shigella
infection. This interview will also help prevent others
from getting sick.
|
|
CONSENT
Allow respondent to provide information on behalf of their
spouse or child
|
You may have already been contacted by the health department. I
would like to ask you a few additional questions about your (or
the ill person’s) recent illness and about any exposures you
(or the ill person) may have had before becoming ill. Your help in
the investigation is very important. Your participation is
voluntary, and you may refuse to answer any question at any time.
All information will be kept confidential to the extent permitted
by law. No names or other identifying information will be used in
any reports. This interview will likely take about 25 to 30
minutes. Are you willing to participate?
If yes:
Thank you. [Proceed to Section 2]
If no: Thank
you for your time. Would you like any additional materials about
Shigella or can I answer any questions for you? If you wish
at any time to complete the questionnaire, please call <health
department phone number>.
|
|
SECTION 1. INTERVIEW INFORMATION
|
Section 1: INTERVIEW
INFORMATION
|
PulseNet
ID #:____________________________
|
WGS
ID #: ____________________________
|
Interviewer
information Name: ________________________________
Agency or organization: ________________________
|
Reporting
state: ___________
|
Reporting
county: ___________
|
Language
interview conducted in: ☐English
☐Spanish
☐Other
(specify):______________
|
Respondent
was: ☐
Self ☐
Parent ☐
Spouse ☐
Other (specify): _______________
|
|
|
SECTION 2. CASE INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
For the first few questions, I will ask some basic demographic
questions so I can learn more about you (or the ill person).
Section 2: CASE
INFORMATION
|
State
(of residence): _______________
|
County
(of residence): ____________________
|
Age
(of case): __________ ☐
Years
☐
Months
☐
Days
|
What
sex were you (or the ill person) assigned at birth?
☐
Female ☐
Male ☐
Unknown
☐
Refused
|
How do you describe your
(or the ill person’s):
|
Ethnicity?
☐
Hispanic or Latino
☐
Not Hispanic or Latino
|
Race?
(select all
that apply) ☐
American Indian or Alaska Native
☐
Asian
☐
Black or African American
☐ Native
Hawaiian or Pacific Islander ☐
White
☐
Refused
|
If
case is ≥14 years old,
what is your (or the ill person’s) current occupation?
______________________________
|
|
|
SECTION 3. HOUSEHOLD INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
Section 3: HOUSEHOLD
INFORMATION
|
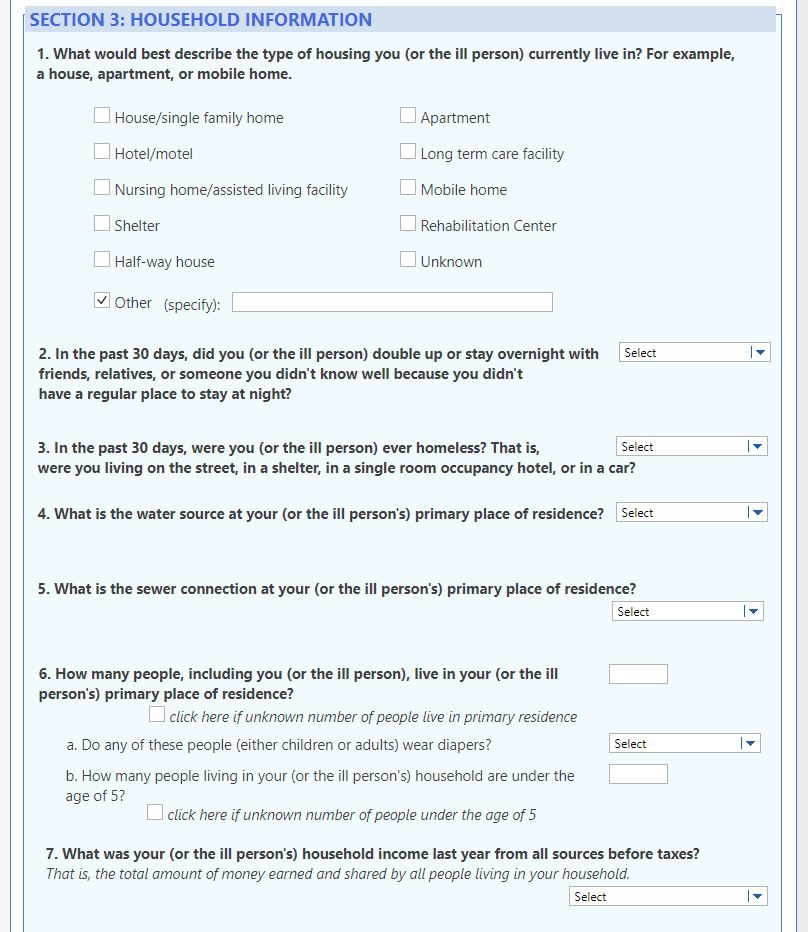
What
would best describe the type of housing you (or the ill
person) currently
live in?
For example, a house, apartment, or mobile home.
☐ House/single
family home ☐
Apartment ☐
Hotel/motel ☐
Long term care facility
☐
Nursing
home/assisted living facility
☐ Mobile
home ☐
Shelter ☐
Rehabilitation center
☐
Half-way house
☐
Unknown ☐
Other (specify): _______________
|
In
the past 30
days, did you
(or the ill person) double up or stay overnight with friends,
relatives, or someone you didn’t know well because you
didn’t have a regular place to stay at night? ☐
Yes ☐
No ☐
Prefer not to
answer ☐
Unknown
|
In
the past 30
days, were
you (or the ill person) ever homeless? That is, were you (or
the ill person) living on the street, in a shelter, in a
single room occupancy hotel, or in a car? ☐
Yes ☐
No ☐
Prefer not to
answer ☐
Unknown
|
What
is the water source at your (or the ill person’s)
primary place of residence?
☐
Municipal
☐
Well
☐
Unknown
☐
Other (specify):
_______________
|
What
is the sewer connection at your (or
the ill person’s)
primary place of residence?
☐
Municipal
☐
Septic
tank ☐
Unknown ☐
Other (specify): _______________
|
How
many people, including you (or
the ill person),
live in your (or
the ill person’s)
primary place of residence? _______
☐
Unknown
Do
any of these people (either children or adults) wear diapers?
☐
Yes ☐
No ☐
Unknown
How
many people living in your (or
the ill person’s)
household are under the age of 5? _______
☐
Unknown
|
What
was your (or the ill person’s) household income last
year from all sources before taxes? That
is, the total amount of money earned and
shared
by
all people living in your
(or
the ill person’s)
household.
☐ <$20,000
☐
$20,000-$39,999
☐
$40,000-$59,999
☐
$60,000-$79,999
☐
$80,000-99,999
☐
$100,000
or more
☐ Prefer
not to answer ☐
Unknown
|
|
|
SECTION 4. CLINICAL INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
Next, I have a few questions about your (or the ill person’s)
recent illness. It may be helpful to have a calendar in front of
you because I will be asking about the dates your (or the ill
person’s) symptoms started and stopped. Do you need some
time to get one?
Section 4: CLINICAL
INFORMATION
|
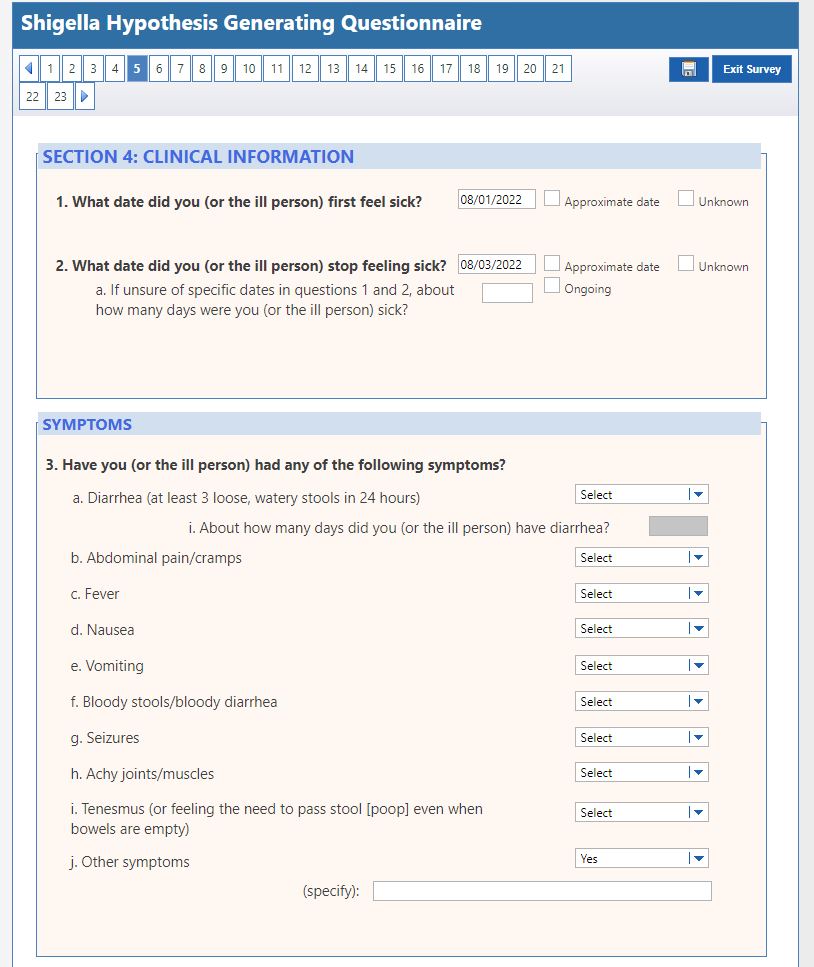
What
date did you (or the ill person) first feel sick? ______
/_____ /_______ ☐
Approximate date
☐
Unknown
Month
/ Day / Year
|
What
date did you (or the ill person) stop feeling sick? ______
/_____ /_______ ☐
Approximate date
☐
Unknown ☐
Ongoing
Month
/ Day / Year
If
unsure of specific dates in questions 1 and 2, about how many
days were you (or the ill person) sick? __________
|
Yes
|
No
|
Don’t
Know
|
Have
you (or the ill person) had any of the following symptoms?
|
☐
|
☐
|
☐
|
Diarrhea
(at least 3 loose, watery stools in 24 hours)
|
|
If
yes to question 3a, about
how many days did you (or the ill person) have
diarrhea?________
|
☐
|
☐
|
☐
|
Abdominal
pain/cramps
|
☐
|
☐
|
☐
|
Fever
|
☐
|
☐
|
☐
|
Nausea
|
☐
|
☐
|
☐
|
Vomiting
|
☐
|
☐
|
☐
|
Bloody
stools/bloody diarrhea
|
☐
|
☐
|
☐
|
Seizures
|
☐
|
☐
|
☐
|
Achy
joints/muscles
|
☐
|
☐
|
☐
|
Tenesmus
(or feeling the need to pass stool [poop] even when bowels are
empty)
|
☐
|
☐
|
☐
|
Other
symptoms I didn’t ask about (specify):
_________________________________________
|
|
|
SECTION 5. MEDICAL CARE AND TREATMENT INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
The next set of questions are about any recent medical care and
treatment you (or the ill person) may have received.
Section 5: MEDICAL
CARE
AND TREATMENT
INFORMATION
|
Yes
|
No
|
Don’t
Know
|
|
☐
|
☐
|
☐
|
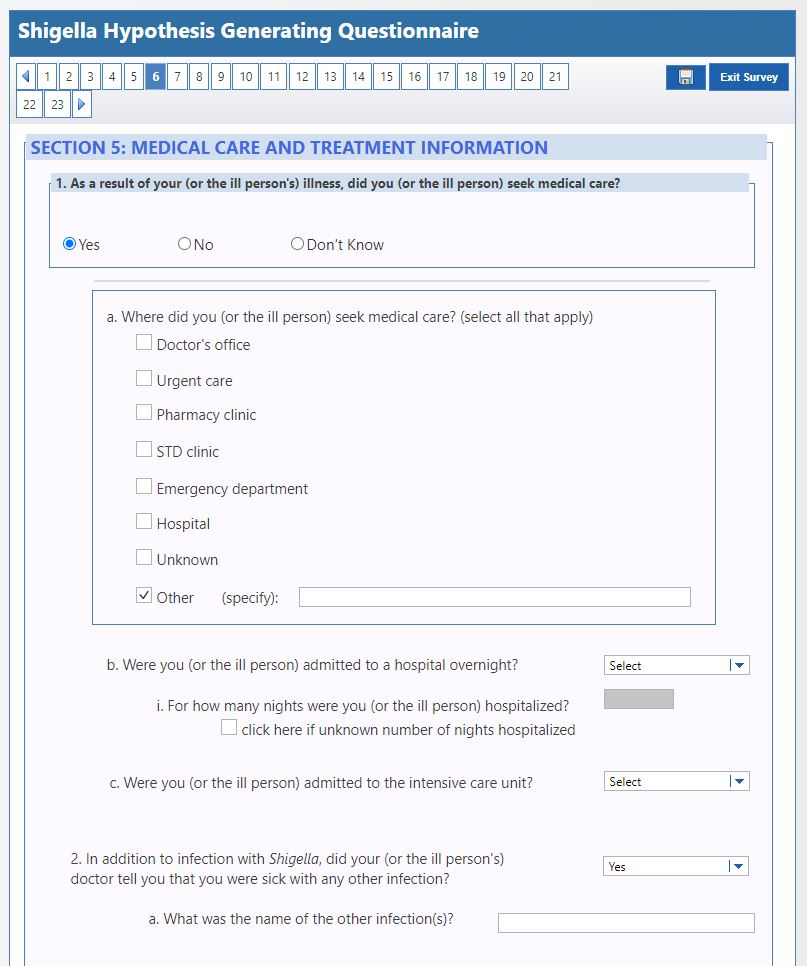
As
a result of your (or the ill person’s) illness, did you
(or the ill person) seek medical care?
|
|
If
yes to question 1, where
did you (or the ill person) seek medical care? (select
all that apply)
☐ Doctor’s
office ☐
Urgent care ☐
Pharmacy clinic
☐
STD clinic
☐
Emergency
department ☐
Hospital
☐
Unknown
☐
Other (specify): _______________
|
☐
|
☐
|
☐
|
If
yes to question 1, were
you (or the ill person) admitted to a hospital overnight?
|
|
If
yes to question 1b,
for how many nights were you (or the ill person)
hospitalized?
_____________
|
☐
|
☐
|
☐
|
If
yes to question 1,
were you (or the ill person) admitted to the intensive care
unit?
|
☐
|
☐
|
☐
|
In
addition to infection with Shigella,
did your (or the ill person’s) doctor tell you that you
were sick with any other infection(s)?
|
|
If
yes to question 2,
what was the name of the other infection(s):
______________________
|
☐
|
☐
|
☐
|
Were
you (or the ill person) prescribed any antibiotics for this
illness? If yes, I will be asking more questions about the
antibiotic, so it may be helpful to get the pill bottles or
packages if available.
|
|
If
yes to question 3, what
was the name of the antibiotic(s), dose, and frequency?
__________________________________________
|
If
yes to question 3, which
date did you (or
the ill person)
start taking the antibiotic(s)?
______
/_____ /_______ ☐
Approximate date
☐
Unknown
Month
/ Day / Year
|
If
yes to question 3, which
date did you (or
the ill person)
stop taking the antibiotic(s)?
______
/_____ /_______ ☐
Approximate date
☐
Unknown ☐
Still
taking antibiotic(s)
Month
/ Day / Year
|
If
yes to question 3,
in the 24 hours
after
taking the antibiotic(s), did your (or
the ill person’s)
symptoms
☐ Get
better/Improve ☐
Stay the Same
☐
Get
Worse
☐
Other
(specify): _____________
|
|
|
SECTION 6. EXPOSURE INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
I would now like to know about your (or your child’s)
recent activities, including travel, events, and contact with
others.
Section 6: EXPOSURE
INFORMATION
|
Yes
|
No
|
Don’t
Know
|
|
☐
|
☐
|
☐
|
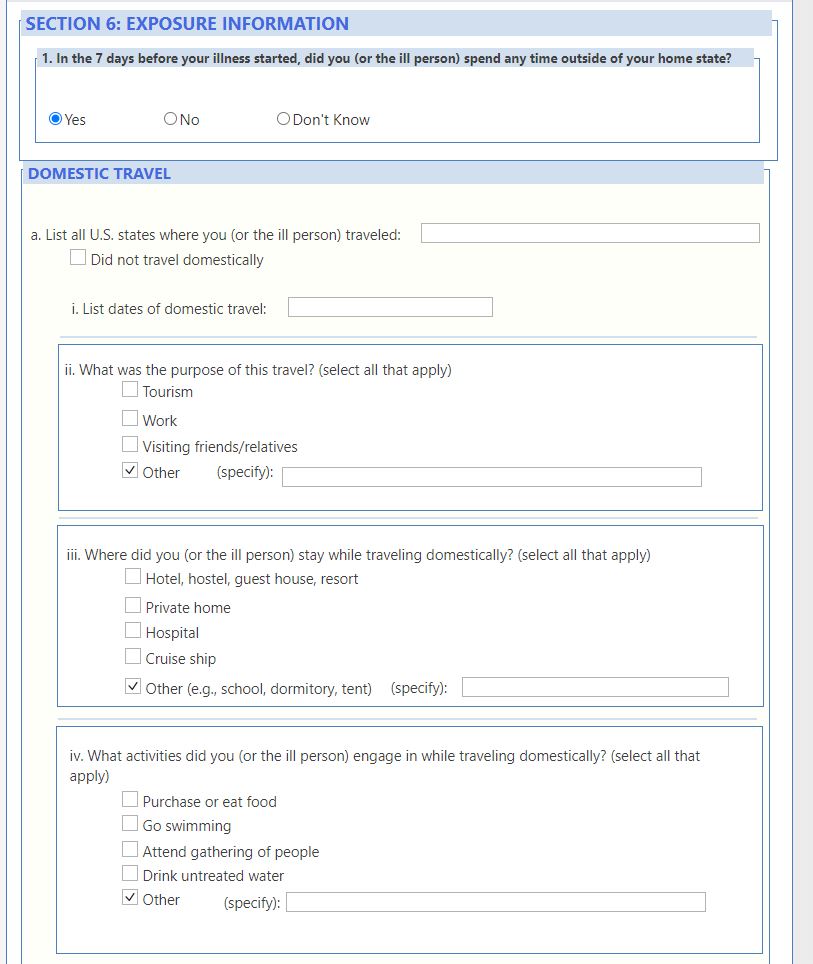
In
the 7
days before
your illness started, did you (or
the ill person)
spend any time outside of your home state?
|
|
If
yes to question 1, list
all U.S. states where you (or the ill person) traveled:
_________________________________________________________
|
List
dates of domestic travel:
___________________________________________
|
What
was the purpose of this travel? (select
all that apply)
☐ Tourism
☐
Work
☐
Visiting
friends/relatives
☐
Other
(specify):________________________
|
Where
did you (or
the ill person)
stay
while traveling domestically? (select
all that apply):
☐ Hotel,
hostel, guest house, resort ☐
Private
home ☐
Hospital
☐
Cruise ship
☐
Other
(e.g., school, dormitory, tent)
(specify):________________________
|
What
activities did you (or the ill person) engage in while
traveling domestically? (select
all that apply)
☐ Purchase
or eat food ☐
Go swimming ☐
Attend gathering of people
☐
Drink
untreated water ☐
Other
(specify):________________________
|
If
yes to question 1,
list all countries outside the United States where you (or the
ill person) traveled:
__________________________________________________
☐
Did not travel internationally
|
List
dates of international travel:
___________________________________________
|
What
was the purpose of this travel? (select
all that apply)
☐ Tourism
☐
Work
☐
Visiting
friends/relatives
☐
Other
(specify):________________________
|
Where
did you (or
the ill person)
stay
while traveling internationally? (select
all that apply):
☐ Hotel,
hostel, guest house, resort ☐
Private
home ☐
Hospital
☐
Cruise ship
☐
Other
(e.g., school, dormitory, tent)
(specify):________________________
|
What
activities did you (or the ill person) engage in while
traveling internationally? (select
all that apply)
☐ Purchase
or eat food ☐
Go swimming ☐
Attend gathering of people
☐
Drink
untreated water ☐
Other
(specify):__________________________
|
☐
|
☐
|
☐
|
In
the past
month, have
you (or the ill person) had contact with any individuals who
traveled outside the United States?
|
|
If
yes to question 2,
where did they travel? (specify):
__________________________________
|
☐
|
☐
|
☐
|
If
yes to question 2,
were they ill with symptoms similar to your (or the ill
person’s) symptoms?
|
☐
|
☐
|
☐
|
If
yes to question 2,
did you (or the ill person) eat any food or drink any
beverages they brought back?
|
|
If
yes to question 2c,
what did you (or the ill person) eat or drink?
(specify):
_______________
|
|
In
the 7 days
before your
(or the ill person’s) illness started, did you (or the
ill person) attend, visit, work in, or volunteer at any of the
following:
|
☐
|
☐
|
☐
|
A
religious gathering (such as church, mosque, or synagogue)?
(specify): _______________
|
☐
|
☐
|
☐
|
Camp?
(specify): _______________
|
☐
|
☐
|
☐
|
Conference
or other large meeting? (specify): _______________
|
☐
|
☐
|
☐
|
Festival,
fair, play, or concert? (specify): _______________
|
☐
|
☐
|
☐
|
Party,
picnic, or barbeque? (specify): _______________
|
☐
|
☐
|
☐
|
Sports
practice, sports game, or exercise class? (specify):
_______________
|
☐
|
☐
|
☐
|
Other
gathering of people I did not ask about? (specify):
_______________
|
Yes
|
No
|
Don’t
Know
|
In
the 7 days
before your
(or the ill person’s) illness started, did you (or the
ill person):
|
☐
|
☐
|
☐
|
Drink
water from an untreated source, such as lake, pond, or river?
(specify): _______________
|
☐
|
☐
|
☐
|
Eat
any foods prepared by a friend, neighbor, or coworker in their
home? (specify): ____________
|
☐
|
☐
|
☐
|
Eat
any foods prepared by a catering company? (such as food served
at a wedding or conference?) (specify): _____________________
|
☐
|
☐
|
☐
|
Eat
at a restaurant? (specify): _____________________
|
☐
|
☐
|
☐
|
Swim
in treated water, such as a swimming pool? (specify):
________________________
|
☐
|
☐
|
☐
|
Swim
in untreated water, such as a lake, river, or ocean?
(specify): __________________
|
☐
|
☐
|
☐
|
Play
in an interactive water fountain, water table, children’s
pool, kiddie pool, or baby pool? (specify): _______________
|
|
In
the 7 days
before your
(or the ill person’s) illness started, did you (or the
ill person) visit, work in, or volunteer at:
|
☐
|
☐
|
☐
|
A
place that serves food, such as a restaurant or cafeteria?
(specify): _______________
|
☐
|
☐
|
☐
|
A
homeless shelter? (specify): _______________
|
☐
|
☐
|
☐
|
A
health care facility? (specify): _______________
|
☐
|
☐
|
☐
|
A
nursing home, long term care, or assisted living facility?
(specify): _______________
|
☐
|
☐
|
☐
|
In
the 7 days
before your
(or the ill person’s) illness started,
did you (or
the ill person)
have contact with someone with diarrhea (at
least 3 loose, watery stools in 24 hours) or
symptoms similar to your (or the
ill person’s)
symptoms?
|
☐
|
☐
|
☐
|
If
yes to question 6, was
this person diagnosed with a Shigella
infection?
|
☐
|
☐
|
☐
|
If
yes to question 6, was
this person a member of your (or
your child’s)
household?
(specify):
_______________
|
☐
|
☐
|
☐
|
If
yes to question 6, does
this person wear diapers?
|
☐
|
☐
|
☐
|
If
yes to question 6e,
did you (or
your child)
change this person’s diapers?
|
|
|
|
While
you (or
the ill person)
were sick
with the Shigella
infection, did you (or the
ill person)
do any of the following:
|
☐
|
☐
|
☐
|
Prepare
or handle food for other people? (specify): _______________
|
☐
|
☐
|
☐
|
Go
swimming or play in a swimming pool, baby pool, interactive
fountain, or water table? (specify): _______________
|
☐
|
☐
|
☐
|
Visit,
work in, or volunteer at a healthcare facility? (specify):
_______________
|
☐
|
☐
|
☐
|
Visit,
work in, or volunteer at a nursing home, long term care, or
assisted living facility? (specify):
_______________
|
☐
|
☐
|
☐
|
Visit,
work in, volunteer, or attend a school or childcare facility?
(specify):
_______________
|
☐
|
☐
|
☐
|
Visit,
work in, volunteer, or attend any gathering of people? For
example, a picnic, party, concert, conference, or religious
gathering. (specify):
_________________________________
|
|
|
SECTION 7. CHILD CARE AND SCHOOL INFORMATION
Allow respondent
to provide information on behalf of their spouse or child
|
We are nearly finished. I have a few questions about your (or
your child’s) recent child care or school attendance.
Section 7: CHILD
CARE
AND
SCHOOL
INFORMATION
|
Yes
|
No
|
Don’t
Know
|
|
☐
|
☐
|
☐
|
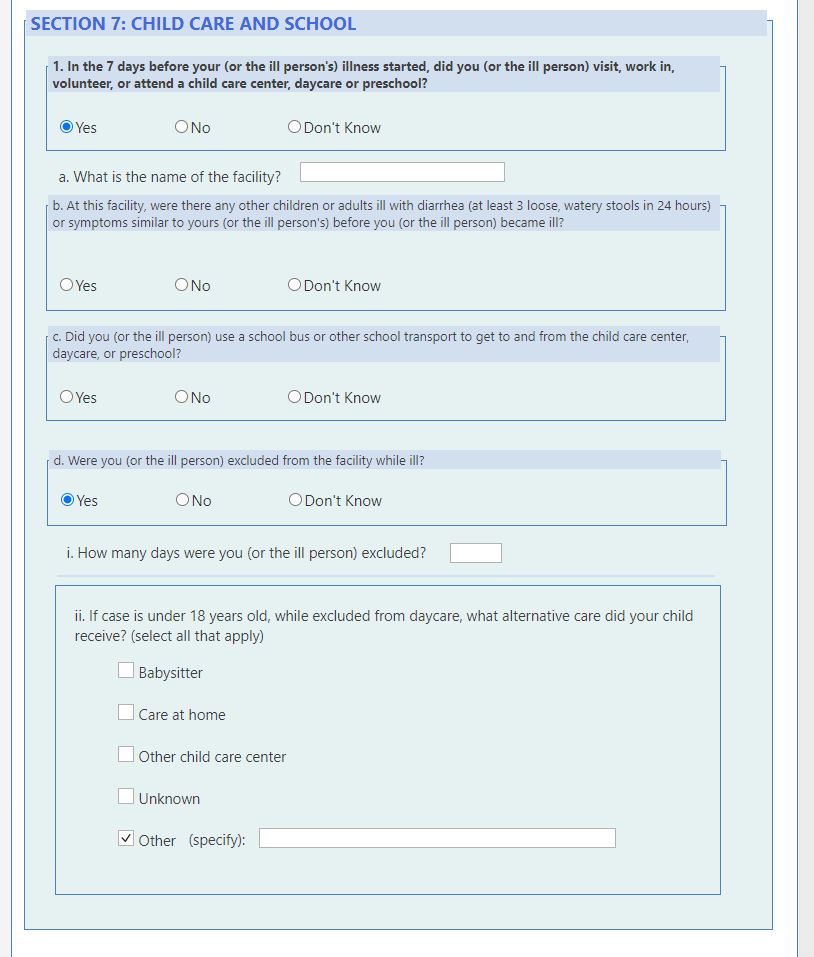
In
the 7 days
before your
(or the ill person’s) illness started, did you (or the
ill person) visit, work in, volunteer, or attend a child care
center, daycare, or preschool?
|
|
If
yes to question 1,
what is the name of the facility?
______________________________
|
☐
|
☐
|
☐
|
If
yes to question 1,
at this facility were there any other children or adults ill
with diarrhea
(at least
3 loose, watery stools in 24 hours) or
symptoms similar to yours (or
the ill person’s)
before you (or
the ill person)
became ill?
|
☐
|
☐
|
☐
|
If
yes to question 1,
did you (or the ill person) use a school bus or other school
transport to get to and from the child care center, daycare,
or preschool?
|
☐
|
☐
|
☐
|
If
yes to question 1,
were you (or the ill person) excluded from this facility while
ill?
|
|
If
yes to question 1d,
how many days were you (or the ill person) excluded?
_______________
|
If
yes to question 1d and case is ≤ 18 years, while
excluded from daycare, what
alternative
care did your child receive? (select
all that apply)
☐ Babysitter
☐
Care
at home
☐
Other
child care center ☐
Unknown
☐
Other
(specify): _______________
|
☐
|
☐
|
☐
|
In
the 7 days
before your
(or the ill person’s) illness started, did you (or the
ill person) attend, visit, work in, or volunteer in a school
(such as an elementary, middle, after school center, or other
type of school)?
|
|
If
yes to question 2,
what is the name of the school?
______________________________
|
☐
|
☐
|
☐
|
If
yes to question 2,
at this school were there any other children or adults ill
with diarrhea
(at
least 3 loose, watery stools in 24 hours) or
symptoms similar to your (or
the ill person’s)
before you became ill?
|
☐
|
☐
|
☐
|
If
yes to question 2,
did you (or the ill person) use a school bus or other
school transport to get to and from the school?
|
☐
|
☐
|
☐
|
If
yes
to
question 2,
were you (or the ill person) excluded from school while
ill?
|
|
If
yes
to
question 2d,
how many days were you (or the ill person) excluded?
_______________
|
If
yes to question 2d and case is ≤ 18 years,
while excluded from school, what
alternative
care did your child receive? (select
all that apply)
☐ Babysitter
☐
Care at home ☐
Self-care ☐
Unknown
☐ Other
(specify): _______________
|
|
|
CONSENT: RECENT SEXUAL ACTIVITY SECTION
|
[Proceed if participant is ≥ 18 years of age and
answering survey on behalf of themself. Otherwise skip section 8
and conclude interview]
Finally, I
would like to ask about your recent sexual activity because
Shigella can be spread through sexual
contact. Shigella germs are very
contagious; it takes just a small number of Shigella
germs to make someone sick. People can get shigellosis when they
put something in their mouths or swallow something that has come
into contact with the stool of someone else who is sick with
shigellosis. This can happen during sex.
As I stated
previously, your responses are voluntary, and you may refuse to
answer any question at any time. We ask all adults who were
diagnosed with a Shigella infection these
questions. Your answers to these questions will be kept private
and may help us to identify how you became sick with a Shigella
infection. This will also help us to prevent others
from getting sick.
Do you wish to
proceed with the next section?
If yes: Thank you [Begin section 8]
If no: That is OK. We appreciate the information
you have given us. ☐
Refused/Prefer Not to Complete
[Skip to Section 9 to close out interview]
|
|
SECTION 8. RECENT SEXUAL ACTIVITY (Only ask if > 18
years of age)
The answer choice
of “Don’t know” for these questions was replaced
with “Prefer not to answer” to more appropriately
reflect answering sensitive questions
|
Section 8: RECENT
SEXUAL ACTIVITY
[Only
ask if ≥
18 years of age]
|
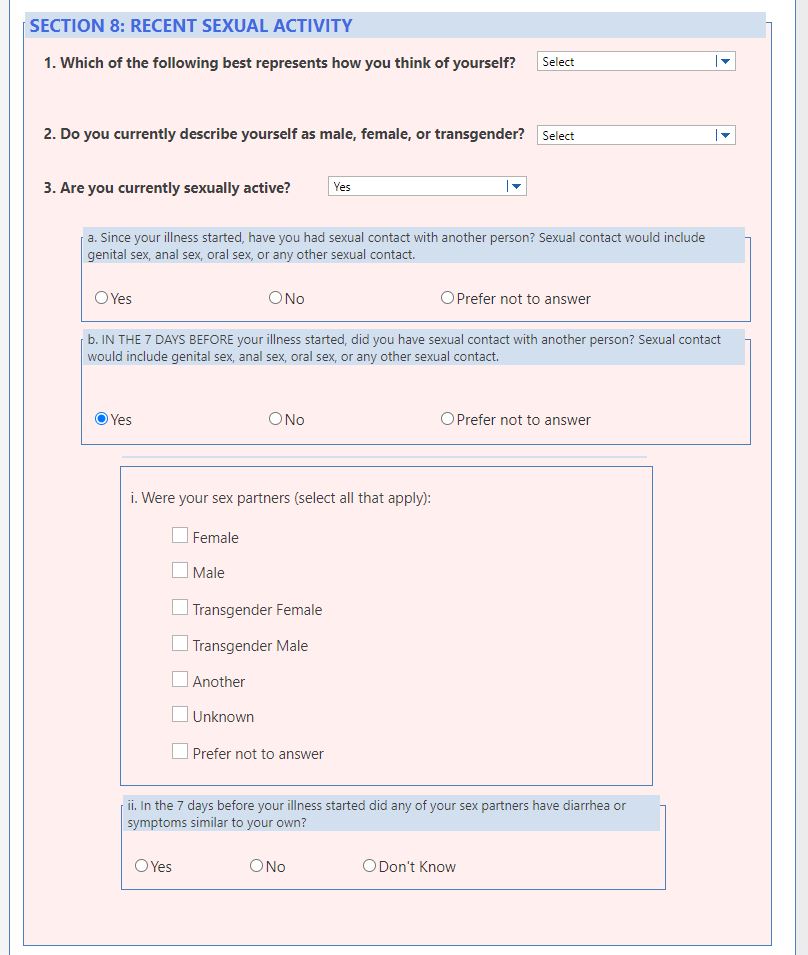
Which
of the following best represents how you think of yourself?
☐ Lesbian
or gay ☐
Straight, that is not lesbian or gay ☐
Bisexual ☐
Something else
(specify): _______________
☐ I
don’t know ☐
Prefer
not to answer
|
Do
you currently describe yourself as male, female, or
transgender?
☐ Male
☐
Female ☐
Transgender ☐
None of these ☐
Prefer not to
answer
|
Yes
|
No
|
Prefer not to answer
|
|
☐
|
☐
|
☐
|
Are
you currently sexually active? (if
no skip to question 4)
|
☐
|
☐
|
☐
|
If
yes to question 3, since
your illness started,
have you had sexual contact with another person? Sexual
contact would include genital sex, anal sex, oral sex, or any
other sexual contact.
|
☐
|
☐
|
☐
|
If
yes to question 3, in
the 7
days before your
illness started, did you have sexual contact with another
person?
Sexual
contact would include genital sex, anal sex, oral sex, or any
other sexual contact.
|
|
If
yes to question 3b, were
your sex partners (select
all that apply):
☐ Female
☐
Male
☐
Transgender
Female ☐
Transgender
Male
☐ Another
☐
Unknown ☐
Prefer Not to
Answer
|
☐
|
☐
|
☐
|
If
yes to question 3b, in
the 7 days
before your
illness started
did any of your sex partners have diarrhea or symptoms
similar to your own?
|
|
If yes to question 3b,
read prompt. For
the next questions I’m going to be more explicit about
the kind of sex you had in the week before your illness
started. This will help me to better understand how you could
have become sick.
|
|
|
|
In
the 7
days before
your illness started, what kind of sexual contact did you
have?
|
☐
|
☐
|
☐
|
Genital
sex (for
example, penis in the vagina)?
|
☐
|
☐
|
☐
|
Anal
sex (for example, penis in the anus)?
|
☐
|
☐
|
☐
|
Oral
sex (for
example, mouth on penis or vagina)?
|
☐
|
☐
|
☐
|
Anilingus
or rimming (meaning mouth on anus)?
|
☐
|
☐
|
☐
|
Other
sexual contact
(for
example touching your partner’s anus with your hands,
your partner touching your anus with their hands, or
sharing of sex toys)?
|
☐
|
☐
|
☐
|
If
yes to question 3b, in
the 7
days before
your illness started did you use drugs or alcohol during or
immediately before sex? Some examples include alcohol,
Viagra, meth, GHB, cocaine, or poppers. (specify):
__________________________________
|
|
In
the 7
days before
your illness, how many sex partners did you have?
(specify):_________
|
☐
|
☐
|
☐
|
If
yes to question 3bv,
were any of these partners new?
|
|
If
yes to question 3bv1, in
the 7
days before
your illness started, did you meet your new sex partner(s)
at any of the following places?
|
☐
|
☐
|
☐
|
Bar,
restaurant or club? (specify): _______________________
|
☐
|
☐
|
☐
|
Bathhouse?
(specify): _______________________
|
☐
|
☐
|
☐
|
Bookstore?
(specify): _______________________
|
☐
|
☐
|
☐
|
Gym?
(specify): _______________________
|
☐
|
☐
|
☐
|
Park?
(specify): _______________________
|
☐
|
☐
|
☐
|
Social
media sites? (specify): _______________________
|
☐
|
☐
|
☐
|
Dating
or hookup sites? (specify): ______________________
|
☐
|
☐
|
☐
|
Party,
conference, or other type of event?
(specify):
______________
|
☐
|
☐
|
☐
|
Sex
club or sex party? (specify): _______________________
|
☐
|
☐
|
☐
|
Other
location I didn’t ask about? (specify):
_______________
|
☐
|
☐
|
☐
|
In
the past
12 months
have you been told by a doctor that you have a sexually
transmitted infection?
|
|
If
yes to question 4,
which infection? (select
all that apply)
☐ Chlamydia
☐
Gonorrhea
☐
Syphilis
☐
Genital warts
☐
Herpes
☐
Other
(specify):_____________
|
|
|
SECTION 9. CLOSING
|
Section 9: CLOSING
|
This is the end of the
questionnaire. Thank you very much for your time.
Would you like any
additional materials about Shigella
or can I answer any questions for you?
|
Thank you for
your time. Have a nice day.
[Conclude
interview]
|
|