Attachment 98 Attachment 98 – MPC Pharmacy Provider Questionnaire
Medical Expenditure Panel Survey (MEPS) COVID-19 Changes
Attachment 98 – MPC Pharmacy Provider Questionnaire
OMB: 0935-0118
Attachment 98
MEDICAL EXPENDITURE PANEL SURVEY
MEDICAL PROVIDER COMPONENT
DATA FORM
FOR
PHARMACIES
for
REFERENCE YEAR 2017
OMB
DCS: READ THIS ALOUD ONLY IF REQUESTED BY RESPONDENT.
PRESS NEXT TO CONTINUE IN THIS EVENT FORM
PRESS BREAKOFF TO DISCONTINUE
(Public reporting burden for this collection of information is estimated to average 3 minutes per response, the estimated time required to complete the survey. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: AHRQ Reports Clearance Officer Attention: PRA, Paperwork Reduction Project (0935-0118) AHRQ, 5600 Fishers Lane, Rockville, MD 20857.)
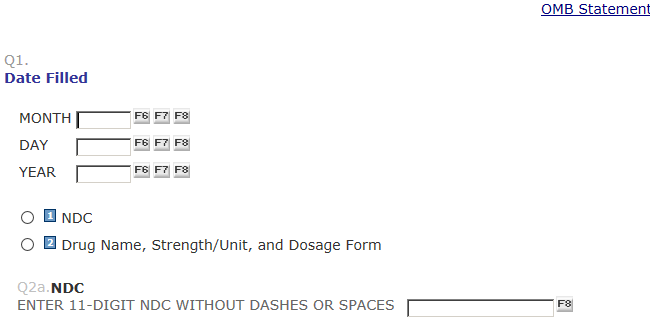
Q1. Date Filled OMB Statement link
MONTH DAY YEAR
Q2. Prescription information will be identified using: 1 = NDC
2 = Drug Name, Strength/Unit, and Dosage Form
NOTE: TRY TO OBTAIN NDC. USE DRUG NAME
ONLY IF NDC NOT AVAILABLE.
Q2a. NDC
ENTER 11-DIGIT NDC WITHOUT DASHES OR SPACES.
NDC IS UNKNOWN OR REFUSED, RETURN TO PREVIOUS SCREEN AND SELECT DRUG NAME OPTION
NDC ROUTE
IF Q2 = 1 (NDC COLLECTED)
The NDC you specified:
NDC: [FILL NDC]
DESCRIPTION: [SMZ/TMP DS TAB 800-160]
DCS: Please confirm that the drug names matches what is in the record (if specified in the record). If it does not, please click on Previous and correct the NDC number entered.
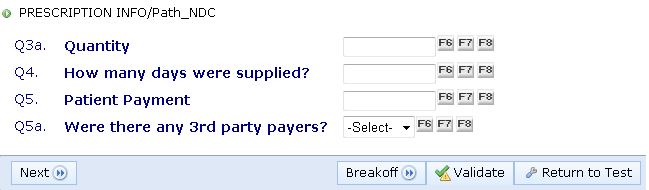
Q3a. Quantity:
Q4. How many days were supplied?
IF PRESCRIPTION WAS TO BE USED “AS NEEDED” ENTER 999

Q5. Patient Payment: $
Q5a. Were there any 3rd party payers? $
DRUG NAME ROUTE
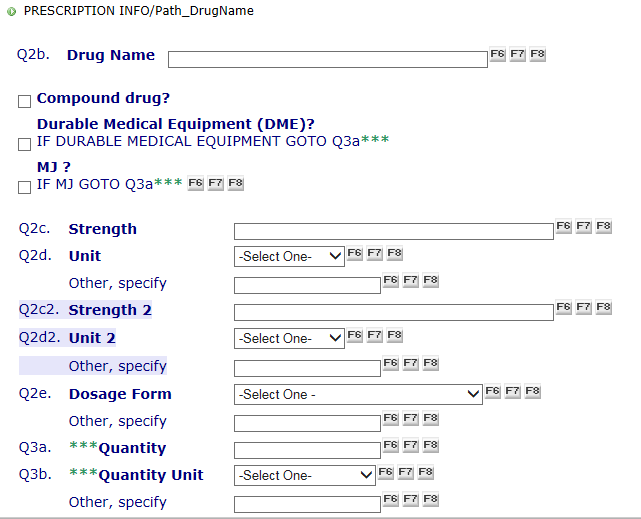
IF Q2 = 3 (DRUG NAME COLLECTED)
Q2b. Drug Name:
Q2b_1
Compound drug?
Durable Medical Equipment
IF DURABLE MEDICAL EQUIPMENT GO TO Q3a***
MJ?
IF MJ GO TO Q3a***
Q2c. Strength
Q2d. Unit:
Q2c1. Strength 2:
Q2d2. Unit 2:
Q2e. Dosage Form:
Q3a. Quantity:
Q3b Unit:
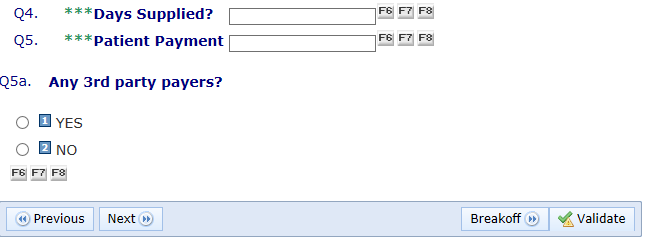
Q4. How many days were supplied?
IF PRESCRIPTION WAS TO BE USED “AS NEEDED” ENTER 999
Q5. Patient Payment: $
Q5a. Were there any 3rd party payers? $
FINAL SCREEN
Q6. Type of 3rd Party Payer
Other Specify Source
Q7. 3rd Party Payment $
NOTE: IF PATIENT PAYMENT WAS $1 OR LESS,
EXPECT THE 3rd PARTY PAYER TO BE A
PUBLIC PROGRAM, E.G., MEDICAID OR
OTHER STATE/LOCAL GOVT, ETC.
Any more 3rd Party Payers?
YES
NO
FINISH SCREEN
PRESS VALIDATE TO COMPLETE THIS EVENT FORM.
Pharmacy
Questionnaire Page
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | 715111: US Public Health Service 1999 Pharmacy Component Data Form |
| Author | MARKOVICH_L |
| File Modified | 0000-00-00 |
| File Created | 2023-08-30 |
© 2026 OMB.report | Privacy Policy