Form Attachment 83 Attachment 83 Attachment 83 – MPC Office-Based Doctor Provider Questio
Medical Expenditure Panel Survey (MEPS) COVID-19 Changes
Attachment 83 – MPC Office-Based Doctor Provider Questionnaire
Office based providers questionnaire
OMB: 0935-0118
Attachment 83
MEDICAL EXPENDITURE PANEL SURVEY
MEDICAL PROVIDER COMPONENT
EVENT FORM
FOR
office-based providers
for
REFERENCE YEAR 2017
SECTION 1 – OMB
DCS: READ THIS ALOUD ONLY IF REQUESTED BY RESPONDENT.
PRESS NEXT TO CONTINUE IN THIS EVENT FORM
PRESS BREAKOFF TO DISCONTINUE
(Public reporting burden for this collection of information is estimated to average 3 minutes per response, the estimated time required to complete the survey. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to: AHRQ Reports Clearance Officer Attention: PRA, Paperwork Reduction Project (0935-0118) AHRQ, 5600 Fishers Lane, Rockville, MD 20857.)
SECTION 2 – VISIT DATE
OMB Statement |
|
B1. What is the (first/next) date of service in your records during this period, for (PATIENT NAME)?
REFERENCE PERIOD – CALENDAR YEAR 2017 |
|
MONTH DAY YEAR |
|
SECTION 2 – LOCATION OF SERVICES RECEIVED
B3. Did (PATIENT NAME) receive the services on (VISIT DATE) in a: |
Physician’s Office; =1 Hospital as an Inpatient; =2 Hospital Outpatient Department; =3 Hospital Emergency Room =4 Somewhere else? =5 IF SOMEWHERE ELSE: Where was that? |
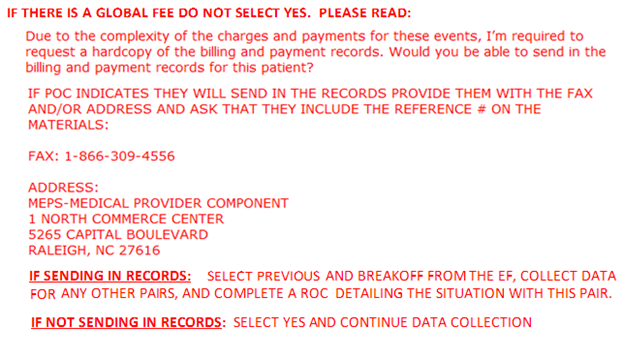
SECTION 3 – GLOBAL FEE
|
|
|
|
|
|
B2a. Was the visit on (VISIT DATE) covered by a global fee, that is, was it included in a charge that covered services received on other dates as well?
EXPLAIN IF NECESSARY: Examples would be a surgeon’s fee covering surgery as well as pre- and post-operative care, or an obstetrician’s fee covering normal delivery as well as pre- and post-natal care.
|
YES=1, NO=2
|
|
B2b. What other dates of service were covered by this global fee? Please include dates before or after 2017 if they were included in the global fee.
ADMINISTER B2c FOR EACH DATE OF SERVICE COVERED BY THE GLOBAL FEE
B2c. Did (PATIENT NAME) receive the services on this date in a: Physician' s Office Hospital as an Inpatient Hospital Outpatient Department Hospital Emergency Room Somewhere else IF SOMEWHERE ELSE: Where was that?
|
MONTH DAY YEAR TYPE SPECIFY: |
|
|
||
|
||
B2d. Do you expect (PATIENT NAME) will receive any future services that will be covered by this same global fee?
|
YES=1, NO=2
|
|
SECTION 4 - DIAGNOSES
B4a. I need the diagnoses for (this visit/these visits). I would prefer the ICD-10 codes, or the DSM-5 codes, if they are available.
IF CODES ARE NOT USED, RECORD DESCRIPTIONS. RECORD UP TO FIVE ICD-10 CODES OR DESCRIPTIONS.
|
ICD-10 CODE DESCRIPTION
|
|
SECTION 5 – SERVICES/CHARGES
B5a. I need to know what services were provided during (this visit/these visits). I would prefer the CPT-4 codes, if they are available.
IF CPT-4 CODES ARE NOT USED, DESCRIBE SERVICES AND PROCEDURES PROVIDED. ENTER UP TO 8 CHARACTERS.
IF CODE BEGINS WITH W, X, Y OR Z, ENTER A DESCRIPTION INSTEAD.
B5b. ASK FOR EACH CPT-4 CODE OR DESCRIPTION: What was the full established charge for this service, before any adjustments or discounts?
IF NO CHARGE: Some facilities that don’t charge for each individual service do associate dollar amounts with services for purposes of budgeting or cost analysis. This is sometimes called a “charge equivalent”. Could you give me the charge equivalent for this service?
NOTE: WE NEVER ENTER $0 FOR A CHARGE IF PROVIDER APPLIED THE CHARGE FOR THIS SERVICE TO SOME OTHER SERVICE, ENTER -4.
C2. [I show the total charges as OUT_TOTLCHRG / I show the charge as undetermined. / I show the charge as OUT_TOTLCHRG, although one or more charges are missing ] Is that correct? IF INCORRECT, CORRECT ENTRIES SHOWN ABOVE AS NEEDED |
CPT-4 CODE DESCRIPTION
|
What was the full established charge, or charge equivalent, for this service?
$
|
|
SECTION 6 – SOURCES OF PAYMENT
C3. Was the practice reimbursed for (this visit/these visits) on a fee-for-service basis or capitated basis? EXPLAIN IF NECESSARY: Fee-for-service means that the practice was reimbursed on the basis of the services provided.
Capitated basis means that the patient was enrolled in a prepaid managed care plan where reimbursement is not tied to specific visits, this is also called Per Member Per Month.
IF IN DOUBT, CODE FEE-FOR-SERVICE. |
Fee-for-service basis =1 Capitated basis =2
|
SECTION 7 – SOURCES OF PAYMENT
C4. From which of the following sources has the practice received payment for (this visit/these visits) and how much was paid by each source? Please include all payments that have taken place between (VISIT DATE) and now for this (visit/these visits).
RECORD PAYMENTS FROM ALL THAT APPLY
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
[DCS ONLY] IF PROVIDER VOLUNTEERS THAT PATIENT PAYS A MONTHLY PREMIUM, VERIFY: So, you receive a monthly payment rather than payment for the specific service? IF YES: GO BACK TO C3 AND CODE AS CAPITATED BASIS.
IF ANY OF THE PAYMENTS IS A LUMP SUM THAT IS NOT YET ALLOCATED, ENTER F8 IN THE APPROPRIATE FIELD(S).
C5. [I show the total payment as TOTPAYM / I show the payment as undetermined. / I show the payment as TOTPAYM, although one or more payments are missing ] Is that correct?
IF NO, CORRECT ENTRIES ABOVE AS NEEDED.
|
SOURCE
a. Patient or Patient’s Family;
b. Medicare;
c. Medicaid;
d. Private Insurance;
e. VA/Champva;
f. Tricare;
g. Worker’s Comp
h. Something else? IF SOMETHING ELSE: What was that?
YES=1, NO=2
|
PAYMENT AMOUNT
|
BOX 1
DO TOTAL PAYMENTS EQUAL TOTAL CHARGES?
YES, AND ALL PAID BY PATIENT OR PATIENT’S FAMILY – 1 (GO TO LSPCHECK)
YES, OTHER PAYERS - 2 (GO TO C5a)
NO, PAYMENTS < CHARGES - 3 (GO TO PLC1)
NO, PAYMENTS > CHARGES - 3 (GO TO ADJEXTRA)
SECTION 8 – VERIFICATION OF PAYMENT
C5a. I recorded that the payment(s) you received equal YES, FINAL PAYMENTS RECORDED IN C4 AND C5 =1
the charge(s). I would like to make sure that I have NO =2
this recorded correctly. I recorded that the total
payment is [SYSTEM WILL DISPLAY TOTAL
PAYMENT FROM C5]. Does this total payment
include any other amounts such as adjustments or
discounts, or is this the final payment?
IF NECESSARY, READ BACK AMOUNT(S)
RECORDED IN C4.
SECTION 9 – PAYMENTS LESS THAN CHARGES
PLC1. It appears that the total payments were less than the total charge. Is that because…
a. There were adjustments or discounts YES=1 NO=2
b. You are expecting additional payment YES=1 NO=2
c. This was charity care or sliding scale YES=1 NO=2
d. This was bad debt YES=1 NO=2
e. Person is an eligible veteran YES=1 NO=2
SECTION 10 – DIFFERENCE BETWEEN PAYMENTS AND CHARGES
Are you expecting additional payment from:
ADJEXTRA It appears that the total payments were more than the total charges. Is that correct?
DCS: IF THE ANSWER IS “NO” PLEASE GO BACK TO C5 (VERIFY TOTAL PAYMENTS) TO RECONFIRM CHARGES AND PAYMENTS AS NEEDED.
YES=1, NO=2
|
Expecting additional payment i. Patient or Patient’s Family? YES=1, NO=2 j. Medicare? YES=1, NO=2 k. Medicaid? YES=1, NO=2 l. Private Insurance? YES=1, NO=2 m. VA/Champva? YES=1, NO=2 n. Tricare? YES=1, NO=2 o. Worker’s Comp? YES=1, NO=2 p. Something else? YES=1, NO=2 IF SOMETHING ELSE: What was that?
|
SECTION 11 – LUMP SUM PAYMENTS
LSPCHECK WAS ANY LUMP SUM ASSOCIATED WITH THE SOURCES OF PAYMENT?
YES
NO
SECTION 12 – CAPITATED BASIS
|
|
C7a. What kind of insurance plan covered the patient for (this visit/these visits)? Was it:
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
|
a. Medicare? YES=1, NO=2 b. Medicaid? YES=1, NO=2 c. Private Insurance? YES=1, NO=2 d. VA/Champva? YES=1, NO=2 e. Tricare? YES=1, NO=2 f. Worker’s Comp? YES=1, NO=2 g. Something else? YES=1, NO=2 IF SOMETHING ELSE: What was that?
|
C7b. Was there a co-payment for (this visit/these visits)?
|
|
C7c. How much was the co-payment? |
$ |
C7d. Who paid the co-payment? Was it:
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
C7e. Do your records show any other payments for (this visit/these visits)?
|
a. Patient or Patient’s Family? YES=1, NO=2 b. Medicare? YES=1, NO=2 c. Medicaid? YES=1, NO=2 d. Private Insurance? YES=1, NO=2 e. Something else?...........................................YES=1, NO=2 (IF SOMETHING ELSE: What was that?)
YES=1, NO=2
|
C7f. From which of the following other sources has the practice received payment for (this visit/these visits) and how much was paid by each source? Please include all adjustment activity that has taken place between (VISIT DATE) and now for (this visit/these visits).
RECORD PAYMENTS FROM APPLICABLE PAYERS.
[DCS ONLY] IF NAME OF INSURER, PUBLIC, OR HMO, PROBE: And is that Medicare, Medicaid, or private insurance?
|
SOURCE a. Patient or Patient’s Family? b. Medicare? c. Medicaid? d. Private Insurance? e. VA/Champva? f. Tricare? g. Worker’s Comp? h. Something else? (IF SOMETHING ELSE: What was that?)
|
PAYMENT AMOUNT
|
BOX 2
BOX 2
IF FEEORCAP = 1 ASK LSPCHECK AND FINISH SCREEN IF FEEOR CAP = 2 GO TO FINISH SCREEN
AFTER VALIDATION USER RETURNS TO CMS AND IS ASKED “ANYMORE EVENTS?”
|
FINISH SCREEN
PRESS VALIDATE TO COMPLETE THIS EVENT FORM.
OBD Questionnaire
Page
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Exhibit 11-2 |
| Author | Doris R. Northrup |
| File Modified | 0000-00-00 |
| File Created | 2022-10-06 |
© 2026 OMB.report | Privacy Policy