MHBG Report
OMB MHBG Report _ Clean 9.21.21_.docx
Community MH Services BG and SAPT BG Application Guidance and Instructions FY 2022-2023
MHBG Report
OMB: 0930-0168
Block Grant Reporting Section
CFDA 93.958
(Mental Health)
U.S. Department of Health and Human Services
Substance Abuse and Mental Health Services Administration
Table of Contents
Introduction
Implementation Report
MHBG Table 1 Priority Area and Annual Performance Indicators – Progress Report
State Agency Expenditure Reports
MHBG Table 2a - (URS Table 7) State Agency Expenditure Report
MHBG Table 2b - (URS Table 7a) - State Agency Early Serious Mental Illness (ESMI) Expenditures Report
MHBG Table 2c - (URS Table 7b) - MHBG State Agency Crisis Services Expenditures Report
MHBG Table 3 - Set-aside for Children’s Mental Health Services
MHBG Table 4 - (URS Table 8) Profile of Mental Health Block Grant Expenditures for Non-Direct Service Activities
MHBG Table 5 - (URS Table 10) - Profiles of Agencies Receiving Block Grant Funds Directly from the State MHA
MHBG Table 6 - Maintenance of Effort for Statewide Expenditures on Mental Health Services
Population and Services Reports
MHBG Table 7 - (URS Table 1) Profile of the State Population by Diagnosis
MHBG Table 8a and MHBG Table 8b - (URS Tables 2A and 2B) Profile of Persons Served, All Programs by Age, Gender and Race/Ethnicity
MHBG Table 9 - (URS Table 3) Profile of Persons Served In the Community Mental Health Settings, State Psychiatric Hospitals, and Other Settings
MHBG Table 10a and MHBG Table 10b - (URS Tables 5A and 5B) Profile of Clients by Type of Funding Support
MHBG Table 11 - (URS Table 6) Profile of Client Turnover.
MHBG Table 12 - (URS Table 12) State Mental Health Agency Profile.
MHBG Tables 13a and 13b - (URS Tables 14A and 14B) Profile of Persons with SMI/SED Served By Age, Gender, and Race/Ethnicity
MHBG Table 14 - (URS Table 15A) Profile of Persons Served in the Community Mental Health Settings, State Psychiatric Hospitals, and Other Settings for Adults with Serious Mental Illness (SMI) and Children with Serious Emotional Disturbance (SED)
E. Performance Indicators and Accomplishments
MHBG Table 15a - (URS Table 4) Profile of Adult Clients by Employment Status
MHBG Table 15b - (URS Table 4A) Profile of Adult Clients by Employment Status: By Primary Diagnosis Reported (Optional Table)
MHBG Table 16 - (URS Table 9) Social Connectedness and Improved Functioning
MHBG Table 17a - (URS Table 11) Summary Profile of Client Evaluation of Care
MHBG Table 17b - (URS Table 11A) Consumer Evaluation of Care by Consumer Characteristics: Race/Ethnicity (Optional Table)
MHBG Table 18 - (URS Table 15) Living Situation Profile
MHBG Table 19 - (URS Table 16) Profile of Adults with Serious Mental Illnesses and Children with Serious Emotional Disturbances Receiving Specific Services
MHBG Table 19a - (URS Table 16A) Adults with Serious Mental Illnesses and Children with Serious Emotional Disturbances Receiving Evidence Based Services for First Episode Psychosis.
MHBG Table 19b – (URS Table 16B) Adults with Serious Mental Illness and Children with Serious Emotional Disturbances Receiving Crisis Response Services.
MHBG Table 20 - (URS Table 17) Profile of Adults with Serious Mental Illnesses Receiving Specific Services during the Year
MHBG Table 21 - (URS Table 19A) Profile of Criminal Justice or Juvenile Justice Involvement
MHBG Table 22 - (URS Table 19B) Profile of Change in School Attendance
MHBG Table 23a - (URS Table 20A) Profile of Non-Forensic (Voluntary and Civil-Involuntary) Patients Readmission to Any State Psychiatric Inpatient Hospital within 30/180 Days of Discharge
MHBG Table 23b - (URS Table 20B) Profile of Forensic Patients Readmission to Any State Psychiatric Inpatient Hospital within 30/180 Days of Discharge
MHBG Table 24 - (URS Table 21) Profile of Non-Forensic (Voluntary and Civil-Involuntary Patients) Readmission to Any Psychiatric Inpatient Care Unit (State Operated or Other Psychiatric Inpatient Unit) within 30/180 Days of Discharge (Optional Table)
States and jurisdictions are required to complete the reporting document. The reporting document is comprised of the following sections:
Section A. Introduction
Title XIX, Part B, Subpart III of the Public Health Service Act (42 U.S.C. 300x-52(a)), requires the Secretary of the Department of Health and Human Services, acting through the Assistant Secretary of the Substance Abuse and Mental Health Services Administration (SAMHSA), to determine the extent to which states and jurisdictions have implemented the state plan for the prior fiscal year. The purpose of the annual report is to provide information to assist the secretary in making this determination.
Additionally, SAMHSA is directed by Congress through the Consolidated Appropriations Act, 2021 and the Coronavirus Response and Relief Supplement Appropriations Act, 2021 [P.L. 116-260], to set aside 5 percent of the Mental Health Block Grant (MHBG) allocation for each state to support evidence-based crisis systems. States are required to provide services to those in crisis through three core services. SAMHSA will collect related data in Sections C and E.
States and jurisdictions are required to prepare and submit their reports for the last completed state fiscal year (SFY), in the format provided in this guidance. The report will address the purposes for which the MHBG funds are expended, the recipients of grant funds, and the authorized activities conducted, and services purchased with such funds. Particular attention should be given to the progress made toward accomplishing the goals and performance indicators identified in the states and jurisdictions’ plans.
All states and jurisdictions are required to prepare and submit their respective reports utilizing SAMHSA’s Web Block Grant Application System (BGAS). This report must be received by SAMHSA no later than December 1, in order for the state or jurisdiction to receive its next grant. If the due date falls on a weekend or federal holiday, the report will be due on the next business day. The following schedule includes specific due dates for annual reports:
Due Dates for Mental Health and Combined Block Grant Components |
||||
FY the state is applying for funds |
Application Due |
Plan Due |
Planning Period |
MHBG Report Due |
2022 |
9/1/2021 |
Yes |
7/1/19 – 6/30/21 |
12/1/2021 Report year is Last Completed SFY |
2023 |
9/1/2022 |
No |
Updates only |
12/1/2022 Report year is Last Completed SFY |
Section B: Implementation Report - In this section states and jurisdictions are required to provide a brief review of the extent to which their respective plans were implemented, the progress towards the priorities and goals identified in the Block Grant plan over the last completed fiscal year. The report should also include a brief review of areas the state or jurisdiction identified in that Block Grant Plan as needing improvement and changes the state or jurisdiction would propose to achieve the goals established in the priorities.
Section C: State Agency Expenditure Reports - In this section states and jurisdictions should provide information regarding expenditures for authorized activities and services for mental health- including crisis services.
Section D: Populations and Services Report - In this section states and jurisdictions must provide specific information regarding the number of individuals served that are the focus of the state’s Mental Health Bock Grant plan. States should report all mental health clients whose care is funded by MHBG, state funds, and any other funds the SMHA considers part of their behavioral health system. In addition, states and jurisdictions should provide specific information regarding the services these individuals received.
Section E: Performance Indicators and Accomplishments - In this section states and jurisdictions are required to complete the Performance Indicator tables. Performance indicators should be reported using the table format provided in this document. The purpose of the performance indicator tables is to show progress made over time as measured by SAMHSA’s National Outcome Measures (NOMS) for mental health services including any state or jurisdiction-selected performance indicators.
B. Implementation Report
The information states and jurisdictions entered into the performance indicator tables (Plan Table 1) in the planning section of the 2022/2023 Behavioral Health Assessment and Plan will automatically populate cells 1 – 6 in the progress report tables below. States and jurisdictions are required to indicate whether each year performance target/outcome measurement identified in the 2022/2023 Plan was “Achieved” or “Not Achieved” in Cell 7, Report of Progress toward Goal Attainment. If a target was not achieved, a detailed explanation must be provided and remedial steps proposed to meet the target.
MHBG Table 1 - Priority Area and Annual Performance Indicators – Progress Report
Priority Areas and Annual Performance Indicators |
|
1. Priority Area: |
|
3. Population(s) (SMI, SED, ESMI, PWWDC, IVDUs, HIV/EIS, TB, OTHER): |
|
|
|
5. Objective: |
|
6. Strategies to attain the objective: |
|
7. Annual Performance Indicators/objectives to measure goal success: |
|
Indicator #1: |
|
|
|
|
|
|
|
|
|
|
|
|
|
8. Report of Progress toward Goal Attainment:
First-year Target: ____ Achieved _____ Not Achieved (If not achieved, explain why.) |
|
Reason why target was not achieved, and changes proposed to meet target:
|
|
C. State Agency Expenditure Reports
States and jurisdictions should provide information regarding MHBG, Medicaid, other federal funding sources, state, local and other funds expended for authorized activities to treat mental illness during the last completed SFY.
Please Note: Data for all tables contained in the Uniform Reporting System (URS) will continue to be submitted into the URS database maintained by the URS Contractor. Please complete the tables described below.
MHBG Table 2a (URS Table 7) - State Agency Expenditure Report. MHBG Table 2 provides information on Mental Health Expenditures and Sources of Funding. This includes funding from Medicaid, the MHBG and other federal funding sources, state, local and other funds.
MHBG Table 2b - State Agency Early Serious Mental Illness (ESMI) Expenditures Report. MHBG Table 2b provides information on Mental Health Expenditures and Sources of Funding specifically for the First Episode Psychosis (FEP) Programs as well as other Early Serious Mental Illness (ESMI) programs through the required MHBG 10% set-aside. This includes funding from Medicaid, the MHBG and other federal funding sources, state, local and other funds. The inclusion of local funds is important but optional.
MHBG Table 2c - MHBG State Agency Crisis Services Expenditures Report. MHBG Table 2c provides information on how different funding sources are being used to fund crisis response services in the state.
MHBG Table 3 - Set-aside for Children’s Mental Health Service. MHBG Table 3 provides a report of statewide expenditures for children’s mental health services during the last completed SFY. States are required to provide systems of integrated services for children with SED. Each year the state shall expend not less than the amount expended in FY 1994. If there is a shortfall in funding available for children’s mental health services, the state may request a waiver. A waiver may be granted if the Secretary determines that the state is providing an adequate level of comprehensive community mental health services for children with SED, as indicated by comparing the number of children in need of such services with the services actually available within the state. The Secretary shall approve or deny the request for a waiver no later than 120 days after the request is made. A waiver granted by the Secretary shall be applicable only for the fiscal year in question.
MHBG Table 4 (URS Table 8) - Profile of Mental Health Block Grant Expenditures for Non-Direct Service Activities. MHBG Table 4 is used to report expenditures of MHBG funds for non-direct service activities that are funded or conducted by the State Mental Health Authority (SMHA) during the last completed SFY.
MHBG Table 5 (URS Table 10) - Profiles of Agencies Receiving Block Grant Funds Directly from the state MHA. MHBG Table 5 reports payments to recipients of MHBG funds including intermediaries, (e.g., administrative service organizations, and other organizations), which provided mental health services during the last completed SFY, including services for those with a first episode psychosis (FEP) and early serious mental illness (ESMI) programs.
MHBG Table 6 - Maintenance of Effort for Statewide Expenditures for Mental Health Service: MHBG Table 6 reports expenditures of all statewide, non-Federal expenditures for authorized activities to treat mental illness during the last completed SFY.
MHBG Table 2a (URS Table 7) - State Agency Expenditure Report
This table describes expenditures for public mental health services provided by mental health providers funded by the state mental health agency by source of funding.
State Agency Expenditures Report |
||||||||||
MHBG Table 2a |
||||||||||
Report Period- From: |
To: |
|||||||||
State Identifier: |
||||||||||
Source of Funds |
||||||||||
Activity (See instructions for using Row 1.) |
A. Substance Abuse Block Grant |
B. Mental Health Block Grant |
C. Medicaid (Federal, State, and Local) |
D. Other Federal Funds (e.g., ACF (TANF), CDC, CMS (Medicare) SAMHSA, etc.)
|
E. State Funds
|
F. Local Funds (excluding local Medicaid) |
G. Other
|
H. COVID-19 Relief Funds (MHBG) a |
I. ARP Funds b |
|
|
|
|||||||||
|
|
|||||||||
|
|
|||||||||
2. Primary Prevention |
|
|
|
|
|
|
|
|
||
a. Substance Abuse Primary Prevention |
|
|
|
|
|
|
|
|
||
b. Mental Health Primary Prevention c |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
3. Evidence-Based Practices for Early Serious Mental Illness including First Episode Psychosis (10 percent of total award MHBG) d. |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
|
|
|||||||||
5. Early Intervention Services for HIV |
|
|||||||||
6. State Hospital |
|
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
7. Other Psychiatric Inpatient Care |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
8. Other 24-Hour Care (Residential Care) |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
9. Ambulatory/Community Non-24-Hour Care |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
10. Administration (Excluding Program and Provider Level) MHBG and SABG must be reported separately e |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
11. Crisis Services (5 percent set-aside) f |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
12. Subtotal (Rows 1, 2, 4, 5 and 9) |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
13. Subtotal (Rows 3, 6, 7 and 8) |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
14. Total |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
a The 24-month expenditure period for the COVID-19 Relief supplemental funding is March 15, 2021 – March 14, 2023, which is different from the expenditure period for the “standard” MHBG. Per the instructions, the standard MHBG expenditures captured in Columns A – G are for the state expenditure period of July 1, 2022 –
June 30, 2024, for most states. Column H should reflect the spending for the state reporting period. The total may reflect the COVID-19 Relief allotment portion used during the state reporting period.
b The expenditure period for The American Rescue Plan Act of 2021 (ARP) supplemental funding is September 1, 2021 – September 1, 2025, which is different from the expenditure period for the “standard” MHBG. The standard MHBG expenditures captured in Columns A – G are for the state expenditure period of July 1, 2022 –
June 30, 2024, for most states.” Column I should reflect the spending for the state reporting period. The total may reflect the ARP allotment portion used during the state reporting period.
c While the state may use state or other funding for these services, the MHBG funds must be directed toward adults with SMI or children with SED
d Column 3B should include Early Serious Mental Illness programs funded through MHBG set aside
e Per statute Administrative expenditures cannot exceed 5% of the fiscal year award.
f Row 10 should include Crisis Services programs funded through different funding sources, including the MHBG set aside. States may expend more than 5 percent of their MHBG allocation.
MHBG Table 2b - MHBG State Agency First Episode Psychosis Expenditure Report
MHBG State Agency Early Serious Mental Illness and First Episode Psychosis Expenditures Report |
|||||||
MHBG Table 2b |
|||||||
Report Period- From: |
To: |
||||||
State Identifier: |
|||||||
Source of Funds |
|||||||
Activity (See instructions for using Row 1)
|
A. Mental Health Block Grant |
B. Medicaid (Federal, State, and Local)
|
C. Other Federal Funds (e.g., ACF (TANF), CDC, CMS (Medicare), SAMHSA, etc.) |
D. State Funds
|
E. Local funds (excluding local Medicaid)
|
F. Other
|
|
1. CSC Evidence-Based Practices for First Episode Psychosis*
|
$ |
$ |
$ |
$ |
$ |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.. Training for ESMI |
$ |
$ |
$ |
$ |
$ |
$ |
|
4.. Planning for ESMI |
|
|
|
|
|
|
|
Total |
$ |
$ |
$ |
$ |
$ |
$ |
|
Comments on Data: |
|||||||
|
|||||||
*When reporting CSC Evidence-Based Practices for First Episode Psychosis, report only those programs that are providing all the components of a CSC model. If the state uses only certain components of a CSC model specifically for FEP, please report them in row 2.
Note, the totals for this table should equal the amounts reported on Row 3 (Evidence-Based Practices for Early Serious Mental Illness) on MHBG Table 2a (URS Table 7a)
MHBG Table 2c - MHBG State Agency Crisis Services Expenditures Report
This table describes expenditures for Crisis Response services provided or funded by the state mental health agency by source of funding.
MHBG State Agency Crisis Services Expenditures Report |
||||||||
MHBG Table 2c |
||||||||
Report Period- From: |
To: |
|||||||
State Identifier: |
||||||||
Source of Funds |
||||||||
Services
|
A. Mental Health Block Grant
|
B. Medicaid (Federal, State, and local) |
C. Other Federal Funds (e.g., ACF (TANF), CDC, CMS (Medicare), SAMHSA, etc.)
|
D. State Funds
|
E. Local funds (excluding local Medicaid)
|
F. Other
|
G. Total |
|
1. Call Centers |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
2. 24/7 Mobile Crisis Teams |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
3. Crisis Stabilization Programs |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
4. Training and Technical Assistance |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
5. Strategic Planning and Coordination |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
Total |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
Comments on Data: |
||||||||
|
||||||||
* Mental Health Block Grant funding includes one-time funding i.e.: 5% Crisis Set-Aside, COVID-19, and ARP sources. If the funding source
is not captured in the table, please report the name of 'Other' funding per service under the comments section.
MHBG Table 3 Set-Aside for Children’s Mental Health Services
States and jurisdictions are required to not spend less than the amount expended in FY 1994.
Statewide Expenditures for Children’s Mental Health Services |
|
MHBG Table 3: |
|
State Identifier: |
|
Report Period: From: |
To: |
Actual SFY 1994 |
Actual SFY 2021 |
|
|
MHBG Table 4 (URS Table 8) Profile of Community Mental Health Block Grant Expenditures for Non-Direct Service Activities
This table describes the use of MHBG funds for non-direct service activities that are sponsored or conducted by the State Mental Health Authority.
Please enter the total amount of the block grant expended for each activity.
a The 24-month expenditure period for the COVID-19 Relief supplemental funding is March 15, 2021 – March 14, 2023, which is different from the expenditure period for the “standard” MHBG. Per the instructions, the standard MHBG expenditures captured in Columns A - C are for the state expenditure period of July 1 – June 30 of the same year for most states. Column B should reflect the spending for the state reporting period. The total may reflect the COVID-19 Relief allotment portion used during the state budget reporting period. b The expenditure period for The American Rescue Plan Act of 2021 (ARP) supplemental funding is September 1, 2021 – September 1, 2025, which is different from the expenditure period for the “standard” MHBG. Per the instructions, the standard MHBG expenditures captured in Columns A – C are for the state expenditure period of July 1 – June 30 of the same year, for most states. Column C should reflect the spending for the state reporting period. The total may reflect the ARP allotment portion used during the state reporting period. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
MHBG Table 5 (URS Table 10) Profiles of Agencies Receiving Block Grant Funds Directly from the State MHA
|
Profiles of Agencies Receiving Block Grant Funds Directly from the State MHA |
||||||||||||||||||||
|
MHBG Table 5 |
||||||||||||||||||||
|
State Identifier: |
||||||||||||||||||||
Report Period- From: |
|
To: |
|||||||||||||||||||
|
|
Source of Funds |
|||||||||||||||||||
|
SA Block Grant |
|
MH Block Grant |
|
|||||||||||||||||
A |
B |
B |
D |
E |
F |
G |
H |
I |
J |
||||||||||||
Entity Number |
I-SATS ID (for SABG) |
Area Served (Statewide or Sub-State Planning Area) |
Provider/Program Name |
Street Address |
City |
State |
Zip |
Total Block Grant Funds |
Prevention (other than primary prevention) and Treatment Services |
Pregnant Women and Women with Dependent Children |
Primary Prevention |
Early Intervention Services for HIV |
Total MH Block Grant Funds |
Adults with serious mental illness |
Children with a serious emotional disturbance |
Set-aside for FEP programs |
Set-aside for ESMI programs |
||||
|
|
|
|
|
|
|
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
||||
|
|
|
|
|
|
|
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
||||
Total |
|
|
|
|
|
|
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
||||
MHBG Table 6 Maintenance of Effort for State Expenditures on Mental Health Services
Maintenance of Effort for State Expenditures on Mental Health Services |
|||
MHBG Table 6: |
|||
State Identifier: |
|||
Report Period- From: |
To: |
||
|
|||
Total Expenditures for State: |
|||
Period
A |
Expenditures
B |
B1 (2018) + B2 (2019) 2
C |
|
SFY 2019 (1) |
|
|
|
SFY 2020 (2) |
|
|
|
SFY 2021 (3) |
|
|
|
Are the expenditure amounts reported in Column B “actual” expenditures for the fiscal years involved?
|
Yes |
No |
SFY 2019 |
|
|
SFY 2020 |
|
|
SFY 2021 |
|
|
If any estimated expenditures are provided, please indicate when “actual” expenditure data will be submitted to SAMHSA: ___/___/_____
mm/dd/yyyy
States are required to submit sufficient information for the Secretary to make a determination of compliance with the statutory Maintenance of Effort (MOE) requirements.1 MOE information is necessary to document that the state maintained expenditures for community mental health services at a level that is not less than the average level of such expenditures for the 2-year period preceding the fiscal year for which the state applies for the grant. The state shall only include community mental health services expenditures for individuals that meet the federal or state definition of SMI adults and SED children. States that received approval to exclude funds from the maintenance of effort calculation should include the appropriate MOE approval documents.
The Secretary may exclude from the aggregate amount any state funds appropriated to the principal agency for authorized activities of a non-recurring nature and for a specific purpose.2
A request for MOE exclusion should meet the following requirements:
The state shall request the exclusion separately from the application.
The request shall be signed by the state’s Chief Executive Officer or by an individual authorized to apply for the CMHS Block Grant on behalf of the Chief Executive Officer.
The state shall provide documentation that supports its position that the funds were appropriated by the state legislature for authorized activities which are of a non-recurring nature and for a specific purpose; indicates the length of time the project is expected to last in years and months; and affirms that these expenditures would be in addition to funds needed to otherwise meet the state’s MOE requirement for the year in which it is applying for exclusion.
The state may not exclude funds from the MOE calculation until such time as the SAMHSA Administrator has approved in writing the state’s request for exclusion.
B. MOE Shortfalls
States are expected to meet the MOE requirement. If a state cannot meet the MOE requirement, the legislation permits relief based on the recognition that extenuating circumstances may explain the shortfall. These conditions are described below.
1. Waiver for Extraordinary Economic Conditions
A state may request a waiver to the MOE requirement if it can be demonstrated that the MOE deficiency was the result of extraordinary economic conditions that occurred during the State Fiscal Year in question. An extraordinary economic condition is defined as a financial crisis in which the total tax revenues declined at least one and one-half percent, and either the unemployment increases by at least one percentage point, or employment declines by at least one and one-half percent.
2. Material Compliance
If the state is unable to meet the requirements for a waiver under extraordinary economic conditions, the authorizing legislation does permit the Secretary, under certain circumstances, to make a finding that even though there was a shortfall on the MOE, the state maintained material compliance with the MOE requirement for the fiscal year in question. Therefore, the state is given an opportunity to submit information that might lead to a finding of material compliance. The relevant factors that SAMHSA considers in making a recommendation to the Secretary include: (1) whether the state maintained service levels; (2) the state’s mental health expenditure history; and (3) the state’s future commitment to funding mental health services.
D. Populations and Services Report
States and jurisdictions are required to provide information regarding individuals that are served by the state mental health authority using MHBG Tables 7 through 14.
MHBG Table 7 (URS Table 1) Profile of the State Population by Diagnosis. MHBG Table 7 provides the number of Adults with serious mental illness (SMI) and Children with serious emotional disturbance (SED) in the reporting year and in three years forward. Data for this table is prepared for the states by SAMHSA.
MHBG Tables 8a and 8b (URS Tables 2A and 2B) Profile of Persons Served, All Programs by Age, Gender and Race/Ethnicity. MHBG Tables 8a and 8b provide an aggregate profile of unduplicated persons in the reporting year. The reporting year should be the latest SFY for which data are available. This profile is based on a client receiving services in programs provided or funded by the state mental health agency. The client profile takes into account institutional and community services for all such programs. States and jurisdictions are to provide this information on all programs by age, gender, and race/ethnicity.
MHBG Table 9 (URS Table 3) Profile of Persons Served in the Community Mental Health Settings, State Psychiatric Hospitals, and Other Settings. MHBG Table 9 provides an aggregate profile of unduplicated persons in the reporting year for services provided or funded through the MHBG. The reporting year should be the latest SFY for which data are available. The client profile considers institutional and community services for all such programs. States and jurisdictions are to provide this information on all programs by age, gender, and race/ethnicity.
MHBG Table 10a and 10b (URS Tables 5A and 5B) Profile of Clients by Type of Funding Support. MHBG Tables 10a and 10b provide the number of female and male clients by race and ethnicity that have Medicaid Only, Non-Medicaid Sources, Both Medicaid and Non-Medicaid, and Status Not Available.
MHBG Table 11 (URS Table 6) Profile of Client Turnover. MHBG Table 11 requests information regarding the profile of client turnover in various out-of-home settings (e.g. state hospitals, inpatient psychiatric hospitals, and residential treatment centers). Information collected by this table requests admissions, discharges, and length of stay.
MHBG Table 12 (URS Table 12) State Mental Health Agency Profile. MHBG Table 12 provides the populations covered in state hospitals and community program in age categories 0-3, 4-17, and 18 and above.
MHBG Tables 13a and 13b (URS Tables 14A and 14B) Profile of Persons with SMI/SED Served By Age, Gender and Race/Ethnicity. MHBG Tables 13a and 13b request counts for persons with SMI or SED using the definitions provided by CMHS. These tables include individuals receiving services in programs provided or funded by the state mental health agency. States and jurisdictions should report using the federal definitions of SMI and SED if they can, if not, please report using the state’s definitions of SMI and SED and provide information in these tables describing your state’s definition.
MHBG Table 14 (URS Table 15A) Profile of Persons Served in the Community Mental Health Settings, State Psychiatric Hospitals, and Other Settings for Adults with SMI and Children with SED. MHBG Table 14 provides a profile for Adults with Serious Mental Illnesses (SMI) and Children With Serious Emotional Disturbances (SED) that received public funded mental health services in community mental health settings, in state psychiatric hospitals, in other psychiatric inpatient programs, and in residential treatment centers for children.
MHBG Table 7 (URS Table 1). Profile of the State Population by Diagnosis |
|||
This table summarizes the estimates of adults residing within the state with serious mental illness (SMI) and children residing within the state with serious emotional disturbances (SED). The table calls for estimates for two time periods, one for the report year and one for three years into the future. CMHS will provide this data to states based on the standardized methodology developed and published in the Federal Register and the state level estimates for both adults with SMI and children with SED. |
|||
|
|||
MHBG Table 7 |
|||
Report Period- From: |
To: |
||
State Identifier: |
|||
|
Current Report Year |
Three Years Forward |
|
Adults with SMI |
|
|
|
Children with SED |
|
|
|
Note: CMHS will complete this table for the states. |
|
||
MHBG Table 8a (URS Table 2A) Profile of Persons Served, All Programs by Age, Gender, Race/Ethnicity |
||||||||||||||||||||||
This table provides an aggregate profile of persons in the reporting year. The reporting year should be the latest state fiscal year for which data are available. This profile is based on a client receiving services in programs provided or funded by the state mental health agency. The client profile takes into account all institutional and community services for all such programs. Please provide unduplicated counts if possible.
|
||||||||||||||||||||||
MHBG Table 8a |
|
|||||||||||||||||||||
Report Period- From: |
To: |
|
||||||||||||||||||||
State Identifier: |
|
|||||||||||||||||||||
|
Total |
American Indian or Alaska Native |
Asian |
Black or African American |
||||||||||||||||||
Female |
Male |
Other |
N/A |
Total |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
||||||
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Age not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Pregnant Women |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Are these numbers unduplicated? |
|
|
|
|
|
|
|
|
|
|
||||||||||||
Comments on Data (for Age): |
|
|
|
|
|
|
|
|
|
|
||||||||||||
Comments on Data (for Gender): |
|
|
|
|
|
|
|
|
|
|
||||||||||||
Comments on Data (for Race/Ethnicity): |
|
|
|
|
|
|
|
|
|
|
||||||||||||
Comments on Data (Overall): |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
(Continued on next page)
MHBG Table 8a (Cont.) |
|
|||||||||||||||||
|
|
|||||||||||||||||
Report Year- From: |
To: |
|||||||||||||||||
State Identifier: |
|
|||||||||||||||||
|
Native Hawaiian or Other Pacific Islander |
White |
More Than One Race Reported |
Race Not Available |
||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
|||
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Age not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pregnant Women |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MHBG Table 8b (URS Table 2B) Profile of Persons Served, All Programs by Age, Gender and Race/Ethnicity
|
Of the total persons served, please indicate the age, gender and the number of persons who are Hispanic/Latino or not Hispanic/Latino. Total persons served would be the total as indicated in MHBG Table 8a. |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
Please report the data under the categories listed - "Total" is calculated automatically.
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
MHBG Table 8b |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
Report Year- From: To: |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
State Identifier: |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
Not Hispanic |
Hispanic or Latino |
Hispanic or Latino Origin Not Available |
Total |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|
|
|
||||||||||||||||||||||||||||||||||||
|
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
Age not available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
Pregnant Women |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
Comments on Data (for Age): |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Comments on Data (for Gender): |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Comments on Data (for Ethnicity): |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Comments on Data (Overall): |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
Are these unduplicated? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
(Continued on next page)
MHBG Table 9 (URS Table 3) Profile of Persons served in the Community Mental Health Settings, State Psychiatric Hospitals and Other Settings
MHBG Table 9 |
|
|||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||
|
Report Year- From: |
To: |
|
|||||||||||||||||||||||||||
|
State Identifier: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
Age 0-17 |
Age 18-20 |
Age 21-64 |
Age 65+ |
|
||||||||||||||||||||||||
|
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
|
|||||||||||||
|
Community Mental Health Programs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
State Psychiatric Hospitals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Other Psychiatric Inpatient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Residential Treatment Centers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Institutions in the Justice System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
(Continued on next page)
MHBG Table 9 (cont.) |
|
|||||||||||
Report Year- From: |
To: |
|
||||||||||
State Identifier: |
|
|||||||||||
Service Setting |
Age Not Available |
Total |
||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|
|||
Community Mental Health Programs
|
|
|
|
|
|
|
|
|
|
|
||
State Psychiatric Hospitals |
|
|
|
|
|
|
|
|
|
|
||
Other Psychiatric Inpatient |
|
|
|
|
|
|
|
|
|
|
||
Residential Treatment Centers |
|
|
|
|
|
|
|
|
|
|
||
Institutions in the Justice System |
|
|
|
|
|
|
|
|
|
|
||
Comments on Data (for Age): |
|
|
|
|
|
|
|
|
|
|
||
Comments on Data (for Gender): |
|
|
|
|
|
|
|
|
|
|
||
Comment on Data (Overall): |
|
|
|
|
|
|
|
|
|
|
||
MHBG Table 10a Profile of Clients by Type of Funding Support (URS Table 5A)
This table provides a summary of clients by Medicaid coverage. Since the focus of the reporting is on clients of the public mental health service delivery system, this table focuses on the clientele serviced by public programs that are funded or operated by the State Mental Health Authority. Persons are to be counted in the Medicaid row if they received a service reimbursable through Medicaid. |
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Please note that the same person may be served in both Medicaid and Non-Medicaid programs during the same reporting period.
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
☐Data Based on Medicaid Services
|
☐Data Based on Medicaid Eligibility, not Medicaid Paid Services
|
☐People Served by Both includes people with any Medicaid
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Race): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (Overall): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Each row should have a unique (unduplicated) count of clients: (1) Medicaid Only, (2) Non-Medicaid Only, (3) Both Medicaid and Other Sources funded their treatment, and (4) Medicaid Status Not Available.
Both includes people with any Medicaid' check box should be checked. |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
(Continued on next page)
MHBG Table 10a (Cont.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Report Period- From: |
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
State Identifier: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
Native Hawaiian or Other Pacific Islander |
White |
More Than One Race Reported |
Race Not Available |
||||||||||||||||||||||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
|||||||||||||||||||||||
Medicaid (only Medicaid) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Non-Medicaid Sources (only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
People Served by Both Medicaid and Non-Medicaid Sources |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Medicaid Status Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Total Served |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
MHBG Table 10b (URS Table 5B) Profile of Clients by Type of Funding Support |
|||||||||||||||||||||||||||||||||||||||||||
Of the total persons covered by Medicaid, please indicate the gender and number of persons who are Hispanic/Latino or not Hispanic/Latino. Total persons covered by Medicaid would be the total indicated in MHBG Table 10a. |
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Please note that the same person may be served in both Medicaid and Non-Medicaid programs during the same reporting period. |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
MHBG Table 10b. |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Report Period- From: |
To: |
|
|||||||||||||||||||||||||||||||||||||||||
State Identifier: |
|
|
|||||||||||||||||||||||||||||||||||||||||
|
Not Hispanic or Latino
|
Hispanic or Latino |
Hispanic or Latino Origin Unknown |
Total |
|||||||||||||||||||||||||||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|||||||||||||||||||||||||||
Medicaid Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Non-Medicaid Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
People Served by Both Medicaid and Non-Medicaid Sources |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Medicaid Status Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Total Served |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Comments on Data (for Ethnicity): |
|
|
|||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|
|
|||||||||||||||||||||||||||||||||||||||||
Comments on Data (Overall): |
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Each row should have a unique (unduplicated) count of clients: (1) Medicaid Only, (2) Non-Medicaid Only, (3) Both Medicaid and Other Sources funded their treatment, and (4) Medicaid Status Unknown. |
|
||||||||||||||||||||||||||||||||||||||||||
MHBG Table 11 (URS Table 6) Profile of Client Turnover |
||||||||||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
MHBG Table 11 |
|
|
|
|
|
|
||||
Report Year- From: |
To: |
|||||||||
State Identifier: |
||||||||||
Profile of Service Utilization |
Total Served at Beginning of Year (unduplicated) |
Admissions During the year (duplicated) |
Discharges During the year (duplicated) |
Length of Stay (in Days): Discharged Patients |
For Clients in Facility for Less Than 1 Year: Length of Stay (in Days): Residents at end of year |
For Clients in Facility More Than 1 Year: Length of Stay (in Days): Residents at end of year |
||||
Average (Mean) |
Median |
Average (Mean) |
Median |
Average (Mean) |
Median |
|||||
State Hospitals |
|
|
|
|
|
|
|
|
|
|
Children (0 to 17 years) |
|
|
|
|
|
|
|
|
|
|
Adults (18 years and over) |
|
|
|
|
|
|
|
|
|
|
Age Not Available |
|
|
|
|
|
|
|
|
|
|
Other Psychiatric Inpatient |
|
|
|
|
|
|
|
|
|
|
Children (0 to 17 years) |
|
|
|
|
|
|
|
|
|
|
Adults (18 years and over) |
|
|
|
|
|
|
|
|
|
|
Age Not Available |
|
|
|
|
|
|
|
|
|
|
Residential Treatment Centers |
|
|
|
|
|
|
|
|
|
|
Children (0 to 17 years) |
|
|
|
|
|
|
|
|
|
|
Adults (18 years and over) |
|
|
|
|
|
|
|
|
|
|
Age Not Available |
|
|
|
|
|
|
|
|
|
|
Community Programs |
|
|
|
|
|
|||||
Children (0 to 17 years) |
|
|
|
|
||||||
Adults (18 years and over) |
|
|
|
|
||||||
Age Not Available |
|
|
|
|
||||||
Comments on Data (State Hospital): |
|
|
|
|||||||
Comments on Data (Other Inpatient): |
|
|
|
|||||||
Comments on Data (Residential Treatment): |
|
|
|
|||||||
Comments on Data (Community Programs): |
|
|
|
|||||||
Comments on Data (Overall): |
|
|
|
|||||||
MHBG Table 12 (URS Table 12) State Mental Health Agency Profile |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
The purpose of this profile is to obtain information that provides a context for the data provided in the tables. This profile covers the populations served, services for which the state mental health agency is responsible, and data reporting capacities especially related to duplication of numbers served as well as certain summary administrative information. |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
|
MHBG Table 12 |
|
|
|
|
|
|
|
|||||||||||
|
Report Year- From: |
To: |
|
|
|
|
|||||||||||||
|
State Identifier: |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
Populations Served |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
1 |
Which of the following populations receive services operated or funded by the state mental health agency? Please indicate if they are included in the data provided in the tables (Check all that apply) |
|
|
|
|
||||||||||||||
|
|
Populations Covered |
Included in Data |
|
|
|
|
||||||||||||
|
State Hospitals |
Community Programs |
State Hospitals |
Community Programs |
|
|
|
|
|||||||||||
|
1. Aged 0 to 3 |
☐Yes |
☐Yes |
☐Yes |
☐Yes |
|
|
|
|
||||||||||
|
2. Aged 4 to 17 |
☐Yes |
☐Yes |
☐Yes |
☐Yes |
|
|
|
|
||||||||||
|
3. Adults Aged 18 and over |
☐Yes |
☐Yes |
☐Yes |
☐Yes |
|
|
|
|
||||||||||
|
4. Forensics |
☐Yes |
☐Yes |
☐Yes |
☐Yes |
|
|
|
|
||||||||||
|
Comments on Data: |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||
2 |
Do all of the adults and children served through the state mental health agency meet the federal definitions of serious mental illness and serious emotional disturbances? |
|
|
|
|
|
|||||||||||||
|
|
☐Serious Mental Illness ☐Serious Emotional Disturbance
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||
2.a. |
If no, please indicate the percentage of persons served for the reporting period who met the federal definitions of serious mental illness and serious emotional disturbance: |
|
|
|
|
|
|||||||||||||
2.a.1 |
Percent of adults meeting federal definition of SMI: |
|
|
|
|
|
|||||||||||||
2.a.2 |
Percentage of children/adolescents meeting federal definition of SED: |
|
|
|
|
|
|||||||||||||
3 Co-Occurring Mental Health and Substance Abuse: |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|||||||||||||||
3.a. |
What percentage of persons served by the SMHA for the reporting period have a dual diagnosis of mental illness and substance abuse? |
|
|
|
|
|
|||||||||||||
3.a.1 |
Percentage of adults served by the SMHA who also have a diagnosis of substance abuse problem: |
|
|
|
|
|
|||||||||||||
3.a.2 |
Percentage of children/adolescents served by the SMHA who also have a diagnosis of substance abuse problem: |
|
|
|
|
||||||||||||||
3.b. |
Percentage of persons served for the reporting period who met the federal definitions of adults with SMI and children with SED have a dual diagnosis of mental illness and substance abuse: |
|
|
|
|
|
|||||||||||||
3.b.1 |
Percentage of adults meeting federal definition of SMI who also have a diagnosis of substance abuse problem: |
|
|
|
|
|
|||||||||||||
3.b.2 |
Percentage of children/adolescents meeting the federal definition of SED who also have a diagnosis of substance abuse problem: |
|
|
|
|
||||||||||||||
3b.3 |
Please describe how you calculate and count the number of persons with co-occurring disorders: |
|
|
|
|
|
|||||||||||||
4 |
State Mental Health Agency Responsibilities |
|
|
|
|
|
|
|
|||||||||||
a. Medicaid: Does the State Mental Health Agency have any of the following responsibilities for mental health services provided through Medicaid? (Check All that Apply) |
|
|
|
|
|
||||||||||||||
1. State Medicaid Operating Agency |
☐Yes |
|
|
|
|
|
|||||||||||||
2. Setting Standards |
☐Yes |
|
|
|
|
|
|||||||||||||
3. Quality Improvement/Program Compliance |
☐Yes |
|
|
|
|
|
|||||||||||||
4. Resolving Consumer Complaints |
☐Yes |
|
|
|
|
|
|||||||||||||
5. Licensing |
☐Yes |
|
|
|
|
|
|||||||||||||
6. Sanctions |
☐Yes |
|
|
|
|
|
|||||||||||||
7. Other |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
Are Data for these programs reported on URS Tables? |
|
|
||||||||||||
b. Managed Care (Mental Health Managed Care |
|
|
|||||||||||||||||
4.b.1 |
Does the state have a Medicaid Managed Care initiative? |
|
|
|
|
||||||||||||||
4.b.2 |
Does the State Mental Health Agency have any responsibilities for mental health services provided through Medicaid Managed Care? |
☐Yes |
☐Yes |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
If yes, please check the responsibilities the SMHA has: |
|
|
|
|
|
|
|
|
|||||||||||
4.b.3 |
Direct contractual responsibility and oversight of the MCOs or BHOs |
☐Yes |
|
|
|
|
|
|
|
|
|||||||||
4.b.4 |
Setting Standards for mental health services |
☐Yes |
|
|
|
|
|
|
|
|
|||||||||
4.b.5 |
Coordination with state health and Medicaid agencies |
☐Yes |
|
|
|
|
|
||||||||||||
4.b.6 |
Resolving mental health consumer complaints |
☐Yes |
|
|
|
|
|
||||||||||||
4.b.7 |
Input in contract development |
☐Yes |
|
|
|
|
|
||||||||||||
4.b.8 |
Performance monitoring |
☐Yes |
|
|
|
|
|
||||||||||||
4.b.9 |
Other |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||
5 |
Data Reporting: Please describe the extent to which your information system allows the generation of unduplicated client counts between different parts of your mental health system. Please respond in particular for MHBG Table 13a and MHBG Table 13b, which require unduplicated counts of clients served across your entire mental health system. |
|
|
|
|
||||||||||||||
Are data reporting in the tables? |
|
|
|
|
|
||||||||||||||
5.a. |
|
☐
|
|
|
|
|
|
||||||||||||
5.b. |
Duplicated: across state hospital and community programs |
|
|
|
|
|
|
||||||||||||
5.c. |
Duplicated: within community programs |
☐ |
|
|
|
|
|
||||||||||||
5.d. |
Duplicated: between Child and Adult Agencies |
☐ |
|
|
|
|
|
||||||||||||
5.e. |
Plans for Deduplication: If you are not currently able to provide unduplicated client counts across all parts of your mental health system, please describe your plans to obtain unduplicated client counts by the end of your Data Infrastructure Grant. |
|
|
|
|
|
|||||||||||||
6 |
Summary Administrative Data |
|
|
|
|
||||||||||||||
6.a. |
Report Year |
|
|
|
|
||||||||||||||
6.b. |
State Identifier |
|
|
|
|
||||||||||||||
Summary Information on Data Submitted by SMHA: |
|
|
|
|
|||||||||||||||
6.c. |
Year being reported: From: |
To |
|
|
|
|
|||||||||||||
6.d. |
Person Responsible for Submission: |
|
|
|
|
||||||||||||||
6.e. |
Contact Phone Number: |
|
|
|
|
||||||||||||||
6.f. |
Contact Address: |
|
|
|
|
||||||||||||||
6.g. |
E-mail:
|
|
|
|
|
||||||||||||||
MHBG Table 13a (URS Table 14A) Profile of Persons with SMI/SED served by Age, Gender and Race/Ethnicity
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This table requests counts for persons with SMI or SED using the definitions provided by SAMHSA. MHBG Table 8a and 8b (URS Table 2A and 2B) included all clients served by publicly operated or funded programs. This table counts only clients who meet the federal definition of SMI or SED. For many states, this table may be the same as MHBG Tables 8a and 8b (URS Table 2A and 2B). States should report using the federal definitions of SMI and SED if they can, if not, please report using your state’s definitions of SMI and SED and provide information below describing your state’s definition. |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Please report the data under the categories listed - "Total" is calculated automatically.
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
MHBG Table 13a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
Report Year- From: |
To: |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
State Identifier: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Total
|
American Indian or Alaska Native |
Asian |
Black or African American |
Native Hawaiian or Other Pacific Islander |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Female |
Male |
Other |
N/A |
Total |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
|
||||||||||||||||||||||||||||||||||||||||||||||
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
Age Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Age): |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Race/Ethnicity): |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (Overall): |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
(Continued on next page)
MHBG Table 13a. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
Report Year: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
State Identifier: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
White |
More Than One Race Reported |
Race Not Available |
|
|
|||||||||||||||||||||||||||||||
|
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
|
|
||||||||||||||||||||||
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Age Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
1. State Definitions Match the Federal Definitions: |
|
|
|
|||||||||||||||||||||||||||||||||
|
☐Yes |
☐No |
Adults with SMI, if No describe or attach state definition: |
|
|
|||||||||||||||||||||||||||||||
☐Yes |
☐No |
|
|
|
||||||||||||||||||||||||||||||||
Diagnoses included in state SMI definition: |
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||
☐Yes |
☐No |
Children with SED, if No describe or attach state definition: |
|
|
||||||||||||||||||||||||||||||||
☐Yes |
☐No |
Diagnoses included in State SED definition: |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
MHBG Table 13b (URS Table 14B) Profile of Persons with SMI/SED Served by Age, Gender and Ethnicity |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Of the total persons served, please indicate the age, gender and the number of persons who meet the federal definition of SMI and SED and who are Hispanic/Latino or not Hispanic/Latino. The total persons served who meet the federal definition of SMI or SED should be the total as indicated in MHBG Table 13b. |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Please report the data under the categories listed - "Total" is calculated automatically. |
|
|
|
|
|
|
|
||||||||||||||||||||||
MHBG Table 13b |
|||||||||||||||||||||||||||||
Report Year- From: |
To: |
||||||||||||||||||||||||||||
State Identifier: |
|||||||||||||||||||||||||||||
|
Not Hispanic or Latino
|
Hispanic or Latino |
Hispanic
or Latino Origin |
Total |
|||||||||||||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|||||||||||||
0-12 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
13-17 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
18-20 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
21-24 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
25-44 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
45-64 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
65-74 years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
75 and older |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Age Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Comments on Data (for Age): |
|||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|||||||||||||||||||||||||||||
Comments on Data (for Race/Ethnicity): |
|||||||||||||||||||||||||||||
Comments on Data (Overall): |
|||||||||||||||||||||||||||||
(Continued on next page)
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
MHBG Table 14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Report Year- From: |
To: |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
State Identifier: |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Age 65+ |
Age Not Available |
Total |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Community Mental Health Programs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
State Psychiatric Hospitals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Other Psychiatric Inpatient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Residential Treatment Centers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Institutions under Justice Systems |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Age): |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on Data (Overall): |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: Clients can be duplicated between rows (e.g., the same client may be served in both state psychiatric hospitals and community mental health centers during the same year and thus would be reported in counts for both rows). |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Instructions: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
1 |
States that have county psychiatric hospitals which serve as surrogate state hospitals should report persons served in such settings as receiving services in state hospitals. |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
2 |
If forensic hospitals are part of the state mental health agency system, include them. |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
3 |
Persons who receive non-inpatient care in state psychiatric hospitals should be included in the Community MH Program Row. |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
4 |
Persons who receive inpatient psychiatric care through a private provider or medical provider licensed, or contracted through the SMHA, should be counted in the "Other Psychiatric Inpatient" row. Persons who receive Medicaid funded inpatient services through a provider that is not licensed or contracted by the SMHA should not be counted here. |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
5 |
A person who is served in both community and inpatient settings should be included in both rows. |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
6 |
RTC: CMHS has a standardized definition of RTC for Children: “An organization, not licensed as a psychiatric hospital, whose primary purpose is the provision of individually planned programs of mental health treatment services in conjunction with residential care for children and youth primarily 17 years old and younger. It has a clinical program that is directed by a psychiatrist, psychologist, social worker, or psychiatric nurse who has a master’s degree or doctorate. The primary reason for the admission of the clients is mental illness that can be classified by either DSM-V or ICD-10 codes other than the codes for mental retardation, developmental disorders, and substance-related disorders such as drug abuse and alcoholism (unless these are co-occurring with a mental illness).” |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
E. Performance Data and Outcomes
MHBG Table 15a (URS Table 4) Profile of Adult Clients by Employment Status. MHBG Table 15a describes the status of adult clients served in the report year by the public mental health system in terms of employment status. The focus is on employment for the working age population, recognizing, however, that there are clients who are disabled, retired or who are homemakers, caregivers, etc., and not a part of the workforce. These persons should be reported under the “Not in Labor Force” category. This category has two subcategories: retired and other (the totals of these two categories should equal the number listed in the "Not in Labor Force" column). Unemployed refers to persons who are looking for work but have not found employment. Data should be reported for clients in non-institutional settings at time of discharge or last evaluation.
MHBG Table 15b (URS Table 4A) Optional Table: Profile of Adult Clients by Employment Status, by Primary Diagnosis Reported. MHBG Table 15b requests information on the status of adult clients served in the report year by the public mental health system in terms of employment status by primary diagnosis reported.
MHBG Table 16 (URS Table 9) Social Connectedness and Improved Functioning. MHBG Table 16 requests states and jurisdictions to provide information for youth and adults regarding social connectedness. In addition, states are required to provide information on functional domains that provide a general sense of an individual’s ability to develop and maintain relationships, cope with challenges, and develop a sense of community belonging.
MHBG Table 17a (URS Table 11) Summary Profile of Client Evaluation of Care. MHBG Table 17a requests information that evaluates the “experience” of care for individuals that participate in the public mental health system. Specifically, the evaluation focuses on several areas including access, quality and the appropriateness of services, participation in treatment planning, and general satisfaction with services. Please provide unduplicated counts, if possible. This table provides an aggregate profile of persons served in the reporting year. The reporting year should be the latest state fiscal year for which data are available. This profile is based on a client's last known living situation.
MHBG Table 17b (URS Table 11A) Optional Table: Consumer Evaluation of Care by Consumer Characteristics: Race/Ethnicity. MHBG Table 17b requests information that evaluates the “experience” of care for individuals that participate in the public mental health system, broken down by race, ethnicity, and age category (adult or child/adolescent).
MHBG Table 18 (URS Table 15), Living Situation Profile. MHBG Table 18 requests information regarding the number of Individuals in Each Living Situation as collected by the most recent assessment in the reporting period. Specifically, information is collected on the individual’s last known living situation. Living situations include, but are not limited to, private residence, foster care, residential care, jail/correctional facility, homeless shelter and other.
MHBG Table 19 (URS Table 11) Profile of Adults with Serious Mental Illness and Children with Serious Emotional Disturbances Receiving Specific Services. MHBG Table 19 requests information regarding the number and demographics of individuals that are receiving specific evidence-based services. In addition, the table requests information on if and how states and jurisdictions monitor the fidelity for the evidence-based services.
MHBG Table 19a (URS Table 16a) Adults with Serious Mental Illness and Children with Serious Emotion Disturbances receiving Evidence Based Services for First Episode Psychosis. Table 19a requests information regarding the number of individuals that are receiving evidence-based services for First Episode Psychosis (FEP). In addition, the table requests information on if, and how, states and jurisdictions monitor the fidelity for the FEP evidence-based services.
MHBG Table 19b Adults with Serious Mental Illness and Children with Serious Emotional Disturbances Receiving Crisis Response Services. Table 19b requests information to assess the usage of crisis response services by adults and children in the state.
MHBG Table 20a (URS Table 16) Profile of Adults with Serious Mental Illnesses and Children with Serious Emotional Disturbances Receiving Specific Services. MHBG Table 20a requests information regarding the number and demographics of individuals that are receiving specific evidence-based services. In addition, the table requests information on if, and how, states and jurisdictions monitor the fidelity for the evidence-based services.
MHBG Table 20b (URS Table 17) Profile of Adults with Serious Mental Illnesses Receiving Specific Services during the Year. MHBG Table 20b provides the number of unduplicated Adults with SMI receiving family psycho education, integrated treatment for co-occurring disorders, illness self-management and medication management.
MHBG Table 21 (URS Table 19A) Profile of Criminal Justice or Juvenile Justice Involvement. MHBG Table 21 requests information to measure the change in arrests over time.
MHBG Table 22 (URS Table 19B) Profile of Change in School Attendance. MHBG Table 22 measures the change in days attended over time. Information required includes information on suspensions, expulsions, and changes in the school attendance.
MHBG Table 23a (URS Table 20A) Profile of Non-Forensic (Voluntary and Civil-Involuntary) Patients Readmission to Any State Psychiatric Inpatient Hospital Within 30/180 Days of Discharge. MHBG Table 23a provides the total number of discharges within the year, the number of readmissions within 30-days and 180-days and the percent readmitted by age, gender, race, and ethnicity.
MHBG Table 23b (URS Table 20B) Profile of Forensic Patients Readmission to Any State Psychiatric Inpatient Hospital within 30/180 Days of Discharge. MHBG Table 23 provides the total number of discharges within the year, the number of readmissions within 30-days and 180-days and the percent readmitted by age, gender, race, and ethnicity.
MHBG Table 24 (URS Table 21) Optional Table: Profile of Non-Forensic (Voluntary and Civil-Involuntary Patients) Readmission to Any Psychiatric Inpatient Care Unit (State Operated or Other Psychiatric Inpatient Unit) within 30/180 Days of Discharge. MHBG Table 24 provides the total number of discharges from inpatient care units within the year, the number of readmissions within 30-days and 180-days and the percent readmitted by age, gender, race, and ethnicity.
MHBG Table 15a (URS Table 4) Profile of Adult Clients by Employment Status |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
This table describes the status of adult clients served in the reporting year by the public mental health system, in terms of employment status. The focus is on employment for the working age population, recognizing, however, there are clients who are disabled, retired, or who are homemakers, caregivers, etc., and not a part of the workforce. These persons should be reported in the “Not in Labor Force” category. This category has two subcategories: retired and other, (the totals of these two categories should equal the number listed in the "Not in Labor Force" column). Unemployed refers to persons who are looking for work but have not found employment. Data should be reported for clients in non-institutional settings at time of discharge or last evaluation. |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
MHBG Table 15a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Report Year- From: |
To: |
||||||||||||||||||||||||||||||||||||
State Identifier: |
|||||||||||||||||||||||||||||||||||||
|
18-20 |
21-64 |
65+ |
Age Not Available |
Total |
||||||||||||||||||||||||||||||||
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Female |
Male |
Other |
N/A |
Total |
|||||||||||||||||
Employed: Competitively Employed Full or Part Time (includes Supported Employment) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Unemployed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Not in Labor Force: Retired, Sheltered Employment, Sheltered Workshops, Other (homemaker, student, volunteer, disabled, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
How Often Does your State Measure Employment Status? |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
What populations are included: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Comments on Data (for Age): |
|
||||||||||||||||||||||||||||||||||||
Comments on Data (for Gender): |
|
||||||||||||||||||||||||||||||||||||
Comments on Data (Overall): |
|
||||||||||||||||||||||||||||||||||||
MHBG Table 15b (URS Table 4A) Optional Table: Profile of Adult Clients by Employment Status: by Primary Diagnosis Reported |
|
|
||||
|
|
|
|
|
|
|
The workgroup exploring employment found that the primary diagnosis of consumer results in major differences in employment status. The workgroup has recommended that we explore the ability of states to report employment by primary diagnosis and the impact of diagnosis on employment. The workgroup recommended 5 diagnostic clusters for reporting. |
||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
MHBG Table 15b |
|
|
|
|
||
Report Year- From: |
To: |
|||||
State Identifier: |
||||||
Clients |
Employed: Competitively Employed Full or Part Time (includes Supported Employment) |
Unemployed |
Not In Labor Force: Retired, Sheltered Employment, Sheltered Workshops, Other (homemaker, student, volunteer, disabled, etc.) |
Employment Status Not Available |
Total |
|
Schizophrenia & Related Disorders (F20, F25) |
|
|
|
|
|
|
Bipolar and Mood Disorders (F30, F31, F32, F33, F34.1, F60.89, F34.0, F32.9) |
|
|
|
|
|
|
Other Psychoses (F22, F23, F24, F29) |
|
|
|
|
|
|
All Other Diagnoses |
|
|
|
|
|
|
No DX and Deferred DX (R69, R99, Z03.89) |
|
|
|
|
|
|
Diagnosis Total |
|
|
|
|
|
|
Comments on Data (for Diagnosis): |
|
|||||
MHBG Table 16 (URS Table 9): SOCIAL CONNECTEDNESS AND IMPROVED FUNCTIONING |
|
|||||||||||
|
|
|||||||||||
|
|
|||||||||||
MHBG Table 16: NOMS Social Connectedness & Functioning |
|
|||||||||||
Report Year (Year Survey was Conducted): |
|
|||||||||||
State Identifier: |
|
|||||||||||
Adult Consumer Survey Results: |
Number of Positive Responses |
Responses |
Percent Positive (calculated) |
|
|
|||||||
1. Social Connectedness |
|
|
|
|
|
|||||||
2. Functioning |
|
|
|
|
|
|||||||
Child/Adolescent Consumer Survey Results: |
Number of Positive Responses |
Responses |
Percent Positive (calculated) |
|
|
|||||||
3. Social Connectedness |
|
|
|
|
|
|||||||
4. Functioning |
|
|
|
|
|
|||||||
Comments on Data: |
|
|
|
|
|
|||||||
Adult Social Connectedness and Functioning Measures |
|
|||||||||||
1. Did you use the recommended new Social Connectedness Questions? ☐Yes ☐No |
|
Measure used |
|
|||||||||
2: Did you use the recommended new Functioning Domain Questions? ☐Yes ☐No |
|
Measure used |
|
|||||||||
3. Did you collect these as part of your MHSIP Adult Consumer Survey? ☐Yes ☐No |
|
|||||||||||
If no, what source did you use? |
|
|||||||||||
Child/Family Social Connectedness and Functioning Measures |
|
|||||||||||
|
|
|
|
|||||||||
4: Did you use the recommended new Social Connectedness Questions? ☐Yes ☐No |
|
Measure used |
|
|||||||||
5: Did you use the recommended new Functioning Domain Questions? ☐Yes ☐No |
|
Measure used |
|
|||||||||
6. Did you collect these as part of your YSS-F Survey? ☐Yes ☐No |
|
|||||||||||
If No, what source did you use? |
|
|||||||||||
Recommended Scoring Rules |
|
|||||||||||
Please use the same rules for reporting Social Connectedness and Functioning Domain scores as for calculating other Consumer Survey Domain scores for Table MHBG Table 18a: e.g.: |
|
|||||||||||
|
||||||||||||
1. Recode ratings of “not applicable” as missing values. |
|
|||||||||||
2. Exclude respondents with more than 1/3 of the items in that domain missing. |
|
|||||||||||
3. Calculate the mean of the items for each respondent. |
|
|||||||||||
4. FOR ADULTS: calculate the percent of scores less than 2.5 (percent agree and strongly agree). |
|
|||||||||||
5. FOR YSS-F: calculate the percent of scores greater than 3.5 (percent agree and strongly agree). |
|
|||||||||||
MHBG Table 17a (URS Table 11): Summary Profile of Client Evaluation of Care |
|
|||||||||||
|
|
|||||||||||
MHBG Table 17a |
|
|||||||||||
Report Year (Year Survey was Conducted): |
|
|||||||||||
State Identifier: |
|
|||||||||||
Adult Consumer Survey Results: |
Number of Positive Responses |
Responses |
Confidence Interval* |
|
||||||||
1. Reporting Positively About Access |
|
|
|
|
||||||||
2. Reporting Positively About Quality and Appropriateness for Adults |
|
|
|
|
||||||||
3. Reporting Positively About Outcomes |
|
|
|
|
||||||||
4. Adults Reporting on Participation in Treatment Planning |
|
|
|
|
||||||||
5. Adults Positively about General Satisfaction with Services |
|
|
|
|
||||||||
|
|
|||||||||||
Child/Adolescent Consumer Survey Results: |
Number of Positive Responses |
Responses |
Confidence Interval* |
|
||||||||
1. Reporting Positively About Access |
|
|
|
|
||||||||
2. Reporting Positively about General Satisfaction for Children |
|
|
|
|
||||||||
3. Reporting Positively about Outcomes for Children |
|
|
|
|
||||||||
4. Family Members Reporting on Participation in Treatment Planning for their Children |
|
|||||||||||
5. Family Members Reporting High Cultural Sensitivity of Staff |
|
|||||||||||
Please enter the number of persons responding positively to the questions and the number of total responses within each group. Percent positive will be calculated from these data. |
|
|||||||||||
* Please report Confidence Intervals at the 95% level. See directions below regarding the calculation of confidence intervals. |
|
|||||||||||
Comments on Data: |
|
|
||||||||||
Adult Consumer Surveys |
|
|||||||||||
1. Was the Official 28 Item MHSIP Adult Outpatient Consumer Survey Used? |
|
|||||||||||
1. a. If no, which version: |
|
|||||||||||
1. Original 40 Item Version |
|
|||||||||||
2. 21-Item Version |
|
|||||||||||
3. State Variation of MHSIP |
|
|||||||||||
4. Other Consumer Survey |
|
|||||||||||
1. b. If other, please attach instrument used. |
|
|||||||||||
1. c. Did you use any translations of the MHSIP into another language? |
|
|||||||||||
2. Other Language: |
|
|||||||||||
Adult Survey Approach: |
|
|||||||||||
2. Populations covered in survey? (Note all surveys should cover all regions of state) |
|
|||||||||||
|
|
|||||||||||
2.a. If a sample was used, what sample methodology was used? |
|
|||||||||||
4. Other Sample: |
|
|
||||||||||
Adult Consumer Surveys (Continued) |
|
|||||||||||
|
|
|||||||||||
2.b Do you survey only people currently in services, or do you also survey persons no longer in service? |
|
|||||||||||
3. Please Describe the populations included in your sample: (e.g., all adults, only adults with SMI, etc.) |
|
|||||||||||
3.4 Other: describe: (for example, if you survey anyone served in the last 3 months, describe that here): |
|
|||||||||||
4. Methodology of collecting data? (Check all that apply) |
|
|
|
|||||||||
|
Self-Administered |
Interview |
|
|
|
|||||||
Phone |
|
|
|
|
|
|||||||
|
|
|
|
|
||||||||
Face-to-face |
|
|
|
|
|
|||||||
Web-Based |
|
|
|
|
|
|||||||
4.b Who administered the Survey? (Check all that apply) |
|
|
|
|||||||||
|
6. Other: describe: |
|
||||||||||
5. Are Responses Anonymous, Confidential, or Linked to other Patient Databases? |
|
|||||||||||
6. Sample Size and Response Rate: |
|
|||||||||||
6.a How many Surveys were Attempted (sent out or calls initiated)? |
|
|||||||||||
6.b How many survey Contacts were made? (surveys to valid phone numbers or addresses) |
|
|||||||||||
6.c How many surveys were completed? (survey forms returned or calls completed) |
|
|||||||||||
6.d What was your response rate? (number of Completed surveys divided by number of Contacts) |
|
|||||||||||
6.e If you receive "blank" surveys back from consumers (surveys with no responses on them), did you count these surveys as "completed" for the calculation of response rates? |
|
|||||||||||
7. Who Conducted the Survey? |
|
|||||||||||
7.a SMHA Conducted or contracted for the Survey (survey done at state level) |
|
|||||||||||
7.b Local Mental Health Providers/County mental health providers conducted or contracted for the survey |
|
|||||||||||
(survey was done at the local or regional level) |
|
|||||||||||
7.c Other: Describe: |
|
|
||||||||||
* Report Confidence Intervals at the 95 percent confidence level |
|
|||||||||||
Note: The confidence interval is the plus-or-minus figure usually reported in newspaper or television opinion poll results. For example, if you use a confidence interval of 4 and 47 percent of your sample picks an answer you can be "sure" that if you had asked the question of the entire relevant population between 43 percent (47-4) and 51 percent (47+4) would have picked that answer. The confidence level tells you how sure you can be. It is expressed as a percentage and represents how often the true percentage of the population who would pick an answer lies within the confidence interval. The 95 percent confidence level means you can be 95 percent certain; the 99 percent confidence level means you can be 99 percent certain. Most researchers use the 95 percent confidence level. When you put the confidence level and the confidence interval together, you can say that you are 95 percent sure that the true percentage of the population is between 43 percent and 51 percent. (From www.surveysystem.com) |
|
|||||||||||
|
|
|||||||||||
Child/Family Consumer Surveys |
|
|||||||||||
1. Was the MHSIP Children/Family Survey (YSS-F) Used? |
|
|||||||||||
If No, what survey did you use? |
|
|||||||||||
If no, please attach instrument used. |
|
|||||||||||
1.c Did you use any translations of the Child MHSIP into another language? |
|
|||||||||||
2. Other Language: |
|
|||||||||||
Child Survey Approach: |
|
|||||||||||
2. Populations covered in survey? (Note: all surveys should cover all regions of state) |
|
|||||||||||
2.a If a sample was used, what sample methodology was used? |
|
|||||||||||
4. Other Sample: |
|
|||||||||||
2.b Do you survey only people currently in services, or do you also Survey Persons no longer in service? |
|
|||||||||||
2a. If yes to 2, please describe how your survey persons no longer receiving services. |
|
|||||||||||
3. Please Describe the populations included in your sample: (e.g., all children, only children with SED, etc.) |
|
|||||||||||
3.4 Other: describe: (for example, if you survey anyone served in the last 3 months, describe that here): |
|
|||||||||||
4. Methodology of collecting data? (Check all that apply) |
|
|||||||||||
|
Self-Administered |
Interview |
|
|
|
|||||||
Phone |
|
|
|
|
|
|||||||
|
|
|
|
|
||||||||
Face-to-face |
|
|
|
|
|
|||||||
Web-based |
|
|
|
|
|
|||||||
4.b. Who administered the Survey? (Check all that apply) |
|
|||||||||||
6. Other: describe: |
|
|||||||||||
5. Are Responses Anonymous, Confidential, or Linked to other Patient Databases? |
|
|||||||||||
6. Sample Size and Response Rate: |
|
|||||||||||
6.a. How many Surveys were Attempted (sent out or calls initiated)? |
|
|||||||||||
6.b. How many survey Contacts were made? (surveys to valid phone numbers or addresses) |
|
|||||||||||
6.c. How many surveys were completed? (survey forms returned or calls completed) |
|
|||||||||||
6.d. What was your response rate? (number of Completed surveys divided by number of Contacts) |
|
|||||||||||
6.e. If you receive "blank" surveys back from consumers (surveys with no responses on them), did you count these surveys as "completed" for the calculation of response rates? |
|
|||||||||||
|
||||||||||||
7. Who Conducted the Survey? |
|
|||||||||||
7.a. SMHA Conducted or contracted for the Survey (survey done at state level) |
|
|||||||||||
7.b. Local Mental Health Providers/County mental health providers conducted or contracted for the survey (survey was done at the local or regional level) |
|
|||||||||||
|
||||||||||||
7.c. Other: Describe: |
|
|||||||||||
MHBG Table 17b (URS Table 11A) Consumer Evaluation of Care by Consumer Characteristics: (Optional Table by Race/Ethnicity.)
Table
17b.
Report
Year: From:
To:
State
Identifier:
Adult
Consumer
Survey
Results:
*State
used the 2 question version for
Hispanic
Origin
Yes No
Please
check the appropriate box on the left. The "Totals"
formula will automatically adjust to account for which method
your state used to ask about
Hispanic
Origin/Status
Indicators
Total
American
Indian
or
Alaska
Native
Asian
Black
or
African
American
Native
Hawaiian
or
Other
Pacific
Islander
White
More
than
One
Race
Reported
Other/
Not
Available
Hispanic
Origin*
Adult
Consumer
Survey
Results:
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
1.
Reporting
Positively
About
Access.
2.
Reporting
Positively
About
Quality
and
Appropriateness.
3.
Reporting
Positively
About
Outcomes.
4.
Reporting
Positively
about
Participation
in
Treatment
Planning
5.
Reporting
Positively
about
General
Satisfaction
6.
Social
Connectedness
7.
Functioning
Child/Adolescent
Family
Survey
Results:
*State
used the 2 question version for
Hispanic
Origin
Yes No
Please
check the appropriate box on the left. The "Totals"
formula will automatically adjust to account for which method
your state used to ask about
Hispanic
Origin/Status
Indicators
Total
American
Indian
or
Alaska
Native
Asian
Black
or
African
American
Native
Hawaiian
or
Other
Pacific
Islander
White
More
than
One
Race
Reported
Other/
Not
Available
Hispanic
Origin*
Child/Adolescent
Family
Survey
Results:
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
#
Positive
Responses
Reporting
Positively
About
Access.
Reporting
Positively
About
General
Satisfaction
Reporting
Positively
About
Outcomes.
Reporting
Positively
Participation
in
Treatment
Planning
for
their
Children.
Reporting
Positively
About
Cultural
Sensitivity
of
Staff.
6.
Social
Connectedness
7.
Functioning
Comments
on
Data: Please
enter the number of persons responding positively to the
questions and the number of total responses within each group.
Percent
positive will be calculated from these data.


MHBG Table 18 (URS Table 15). Living Situation Profile: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of Clients in Each Living Situation as Collected by the Most Recent Assessment in the Reporting Period |
|
|||||||||||
All Mental Health Programs by Age, Gender, and Race/Ethnicity |
|
|
|
|
|
|
|
|
||||
Please provide unduplicated counts, if possible. This table provides an aggregate profile of persons served in the reporting year. The reporting year should be the latest state fiscal year for which data are available. This profile is based on a client's last known Living Situation. |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
MHBG Table 18 |
|
|
|
|
|
|
|
|
|
|
|
|
Report Year- From: |
To: |
|||||||||||
State Identifier: |
|
|||||||||||
|
Private Residence |
Foster Home |
Residential Care |
Crisis Residence |
Children's Residential Treatment |
Institutional Setting |
Jail/Correctional Facility |
Homeless/ Shelter |
Other |
NA |
Total |
|
0-17 |
|
|
|
|
|
|
|
|
|
|
|
|
18-64 |
|
|
|
|
|
|
|
|
|
|
|
|
65 + |
|
|
|
|
|
|
|
|
|
|
|
|
Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
|
American Indian/Alaska Native |
|
|
|
|
|
|
|
|
|
|
|
|
Asian |
|
|
|
|
|
|
|
|
|
|
|
|
Black/African American |
|
|
|
|
|
|
|
|
|
|
|
|
Hawaiian/Pacific Islander |
|
|
|
|
|
|
|
|
|
|
|
|
White/Caucasian |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
More than One Race Reported |
|
|
|
|
|
|
|
|
|
|
|
|
Race/Ethnicity Not Available |
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
|
(Continued on next page)
MHBG Table 18 (cont.) Living Situation Profile: |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Number of Clients in Each Living Situation as Collected by the Most Recent Assessment in the Reporting Period |
|
|||||||||||||
All Mental Health Programs by Age, Gender, and Race/Ethnicity |
|
|
|
|
|
|
|
|
||||||
Please provide unduplicated counts, if possible. This table provides an aggregate profile of persons served in the reporting year. The reporting year should be the latest state fiscal year for which data are available. This profile is based on a client's last known Living Situation. |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Please report the data under the Living Situation categories listed - "Total" is calculated automatically. |
|
|
|
|
|
|||||||||
MHBG Table 18 |
|
|
|
|
|
|
|
|
|
|
|
|||
Report Year- From: |
To: |
|||||||||||||
State Identifier: |
|
|||||||||||||
|
Private Residence |
Foster Home |
Residential Care |
Crisis Residence |
Children's Residential Treatment |
Institutional Setting |
Jail/ Correctional Facility |
Homeless/ Shelter |
Other |
NA |
Total |
|||
Hispanic or Latino Origin |
|
|
|
|
|
|
|
|
|
|
|
|||
Non-Hispanic or Latino Origin |
|
|
|
|
|
|
|
|
|
|
|
|||
Hispanic or Latino Origin Not Available |
|
|
|
|
|
|
|
|
|
|
|
|||
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
|||
Comments on Data: |
|
|||||||||||||
How Often Does your State Measure Living Situation? |
|
|
|
|
|
|
|
|
||||||
* Hispanic: Only use the "Hispanic" row under Race if data for Hispanic as an Ethnic Origin are not available |
|
|
|
|
|
|
||||||||

MHBG Table 19a Adults with Serious Mental illness and Children with Serious Emotional Disturbances Receiving Evidence-Based Services for First Episode Psychosis.
This table provides the number of Adults with SMI and Children with SED, who were admitted into and received Coordinated Specialty Care (CSC) evidence based First Episode Psychosis Services (FEP). The reporting year should be the latest fiscal year for which data are available.
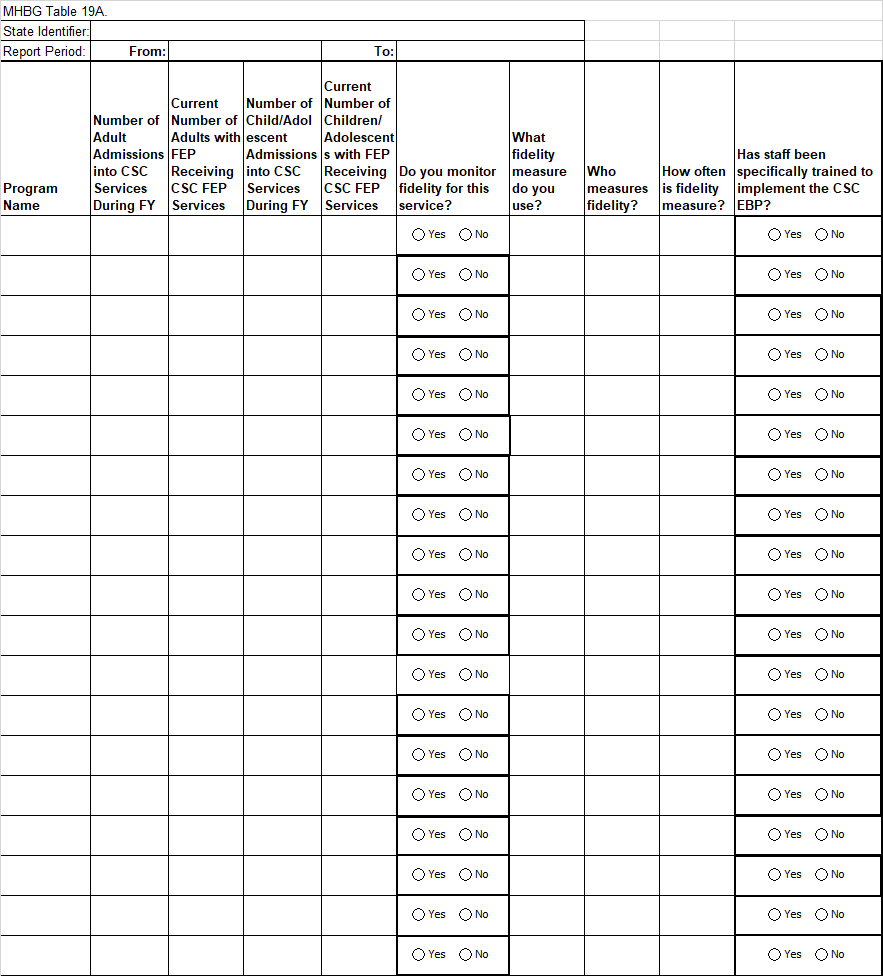
MHBG Table 19b (URS Table 16B) Adults with Serious Mental Illness and Children with Serious Emotional Disturbances Receiving Crisis Response Services.
This table provides the number and percentage of the respective population of adults with serious mental illness and children with serious emotional disturbances that are receiving Crisis Response services. The reporting year should be the latest state fiscal year for which data are available.
Table 16b |
||||
State Identifier: |
|
|||
Report Period |
From: |
|
To: |
|
Service |
Actual Number of Adults Served via Service |
Estimated Percentage of Adult Population with Access to Service |
Actual Number of Children Served via Service |
Estimated Percentage of Child Population with Access to Service |
Call Centers |
|
|
|
|
24/7 Mobile Crisis Teams |
|
|
|
|
Crisis Stabilization Programs |
|
|
|
|
MHBG Table 20 (URS Table 17): Profile of Adults with Serious Mental Illnesses Receiving Specific Services During the Year. |
|||||||||||||||||||||||||
MHBG Table 20 |
|
|
|||||||||||||||||||||||
Report Year- From To: |
|
|
|||||||||||||||||||||||
State Identifier: |
|||||||||||||||||||||||||
|
ADULTS WITH SERIOUS MENTAL ILLNESS |
|
|
||||||||||||||||||||||
|
Receiving Family Psychoeducation |
Receiving Integrated Treatment for Co-occurring Disorders (MH/SA) |
Receiving Illness Self-Management |
Receiving Medication Management |
|||||||||||||||||||||
Age |
|
|
|
|
|||||||||||||||||||||
18-20 |
|
|
|
|
|||||||||||||||||||||
21-64 |
|
|
|
|
|||||||||||||||||||||
65-74 |
|
|
|
|
|||||||||||||||||||||
75+ |
|
|
|
|
|||||||||||||||||||||
Not Available |
|
|
|
|
|||||||||||||||||||||
TOTAL |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
Gender |
|
|
|
|
|||||||||||||||||||||
Female |
|
|
|
|
|||||||||||||||||||||
Male |
|
|
|
|
|||||||||||||||||||||
Other |
|
|
|
|
|||||||||||||||||||||
Not Available |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
Race |
|
|
|
|
|||||||||||||||||||||
American Indian/ Alaska Native |
|
|
|
|
|||||||||||||||||||||
Asian |
|
|
|
|
|||||||||||||||||||||
Black/African American |
|
|
|
|
|||||||||||||||||||||
Hawaiian/Pacific Islander |
|
|
|
|
|||||||||||||||||||||
White |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
More than one race |
|
|
|
|
|||||||||||||||||||||
Unknown |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
Do you monitor fidelity for this service? |
☐Yes ☐No |
☐Yes ☐No |
Yes ☐No |
Yes ☐No |
|||||||||||||||||||||
IF YES, |
|
|
|
|
|||||||||||||||||||||
What fidelity measure do you use? |
|
|
|
|
|||||||||||||||||||||
Who measures fidelity? |
|
|
|
|
|||||||||||||||||||||
How often is fidelity measured? |
|
|
|
|
|||||||||||||||||||||
Have staff been specifically trained to implement the EBP? |
☐Yes ☐No |
☐Yes ☐No |
☐Yes ☐No |
☐Yes ☐No |
|||||||||||||||||||||
|
|||||||||||||||||||||||||
* Hispanic is part of the total served. |
|||||||||||||||||||||||||
Comments on Data (overall): |
|
|
|
||||||||||||||||||||||
Comments on Data (Family Psycho-education): |
|
|
|
||||||||||||||||||||||
Comments on Data (Integrated Treatment for Co-occurring Disorders): |
|
|
|||||||||||||||||||||||
Comments on Data (Illness Self-Management): |
|
|
|
||||||||||||||||||||||
Comments on Data (Medication Management): |
|
|
|
||||||||||||||||||||||
|
|||||||||||||||||||||||||
* Hispanic: Only use the "Hispanic" row under Race, if data for Hispanic as an Ethnic Origin, are not available |
|||||||||||||||||||||||||
MHBG Table 21 (URS Table 19A) Profile of Criminal Justice or Juvenile Justice Involvement.
1. The SAMHSA National Outcome Measure for Criminal Justice measures the change in Arrests over time.
2. If your SMHA has data on Arrest records from alternatives sources, you may also report that here. If you only have data for arrests for consumers in this year, please report that in the T2 columns. If you can calculate the change in Arrests from T1 to T2, please use all those columns.
3. Please complete the check boxes at the bottom of the table to help explain the data sources that you used to complete this table.
4. Please tell us anything else that would help us to understand your indicator (e.g., list survey or MIS questions; describe linking methodology and data sources; specify time period for criminal justice involvement; explain whether treatment data are collected).
-
State: Time period in which services were received: ______________________________
For Consumers in Service for at least 12 months
T1
T2
T1 to T2 Change
Assessment of the Impact of Services
"T1" Prior 12 months
(more than 1 year ago)
"T2" Most Recent 12 months
(this year)
If Arrested at T1 (Prior 12 Months)
If Not Arrested at T1 (Prior 12 Months)
Over the last 12 months, my encounters with the police have…
Arrested
Not
Arrested
No
Response
Not No
Arrested Arrested Response
# with an # with No No
Arrest in T2 Arrest at T2 Response
# with an # with No No
Arrest in T2 Arrest at T2 Response
# Reduced (fewer encounters)
# Stayed the Same
# Increased
# Not
Applicable
No
Response
Total
Responses
Total
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Total Children/Youth (under age 18)
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Female
0
Male
0
Other
Gender NA
0
Total Adults (age 18 and over)
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Female
0
Male
0
Other
Gender NA
0
For Consumers Who Began Mental Health Services during the past 12 months
T1
T2
T1 to T2 Change
Assessment of the Impact of Services
"T1" 12 months prior to beginning services
"T2" Since Beginning Services
(this year)
If Arrested at T1 (Prior 12 Months)
If Not Arrested at T1 (Prior 12 Months)
Since starting to receive MH Services, my encounters with the police have…
Arrested
Not
Arrested
No
Response
Not No
Arrested Arrested Response
# with an # with No No
Arrest in T2 Arrest at T2 Response
# with an # with No No
Arrest in T2 Arrest at T2 Response
# Reduced (fewer encounters)
# Stayed the Same
# Increased
# Not
Applicable
No
Response
Total
Responses
Total
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Total Children/Youth (under age 18)
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Female
0
Male
0
Other
Gender NA
0
Total Adults (age 18 and over)
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Female
0
Male
0
Other
Gender NA
0
|
Please Describe the Sources of your Criminal Justice Data
Source of adult criminal justice information ☐1) Consumer survey (recommended questions) ☐2) Other Consumer Survey: Please send copy of questions ☐3) Mental health MIS ☐4) State criminal justice agency ☐5) Local criminal justice agency ☐6) Other (specify)________________________________ Sources of children/youth criminal justice Information: ☐1) Consumer survey (recommended questions) ☐2) Other Consumer Survey: Please send copy of questions ☐3)Mental health MIS ☐4) State criminal/juvenile justice agency ☐5) Local criminal/juvenile justice agency ☐6) Other (specify)________________________________ |
Measure of adult criminal Involvement: ☐1) Arrests ☐2) Other (specify): |
Measure of children/youth criminal justice Involvement: ☐1) Arrests ☐2) Other (specify): |
Mental health programs included: ☐1)Adults with SMI only ☐2) Other adults (specify)____________________________________ ☐3) Both (all adults) ☐1) Children with SED only ☐2) Other children (specify) ☐3) Both (all children) |
Region for which adult data are reported: ☐1) The whole state ☐2) Less than the whole state (please describe): |
Region for which children/youth data are reported: ☐1) The whole state ☐2) Less than the whole state (please describe): |
What is the Total Number of Persons Surveyed, or for whom Criminal Justice Data are Reported Child/Adolescents Adults 1. If data is from survey, what is the total number of people from which the sample was drawn? 2. What was your sample size (How many individuals were selected for the sample)? 3. How many survey contacts were made (surveys to valid phone numbers or addresses)? 4. How many surveys were completed (survey forms returned or calls completed), if data source was not a survey? How many persons were CJ data available for? 5. What was your response rate? (number of completed surveys divided by number of contacts): |
State Comments/Notes:
|
Instructions:
If you have responses to a survey by person not in the expected age group, you should include those responses with other responses from the survey (e.g., if a 16 or 17 year old responds to the Adult MHSIP survey, please include their responses in the Adult categories, since that was the survey they used). |
Table 22 (URS Table 19b) Profile of Change in School Attendance
1. The SAMHSA National Outcome Measure for School Attendance measures the change in days attended over time. The DIG Outcomes Workgroup pilot tested 3 consumer self-report items that can be used to provide this information. If your state has used the 3
Consumer Self-Report items on School Attendance, you may report them here.
2. If your SMHA has data on School Attendance from alternatives sources, you may also report that here. If you only have data for School attendance for consumers in this year, please report that in the T2 columns. If you can calculate the change in Attendance from T1 to T2, please use all these columns.
3. Please complete the check boxes at the bottom of the table to help explain the data sources that you used to complete this table.
4. Please tell us anything else that would help us to understand your indicator (e.g., list survey or MIS questions; describe linking methodology and data sources; specify time period for criminal justice involvement; explain whether treatment data are collected).
Table22. Profile of Change in School Attendance
State: Time period in which services were received: For Consumers in Service for at least 12 months |
|||||||||||||||||||||
|
T1 |
T2 |
T1 to T2 Change |
Impact of Services |
|||||||||||||||||
"T1" Prior 12 months (more than 1 year ago) |
"T2" Most Recent 12 months (this year) |
If Suspended at T1 (Prior 12 Months) |
If Not Suspended at T1 (Prior 12 Months) |
Over the last 12 months, the number of days my child was in school have |
|||||||||||||||||
# Suspended or Expelled |
# Not Suspended or Expelled |
No Response |
# Suspended or Expelled |
# Not Suspended or Expelled |
No Response |
# with an Expelled or Suspended in T2 |
# with No Suspension or Expulsion at T2 |
No Response |
# with an Expelled or Suspended in T2 |
# with No Suspension or Expulsion at T2 |
No Response |
# Greater (Improved) |
# Stayed the Same |
# Fewer days (gotten worse) |
# Not Applicable |
No response |
Total Responses |
|
|||
Total |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
||
Gender |
|
||||||||||||||||||||
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Gender NA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Age |
|
||||||||||||||||||||
Under 18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
For Consumers Who Began Mental Health Services during the past 12 months |
|||||||||||||||||||||
|
T1 |
T2 |
T1 to T2 Change |
Impact of Services |
|||||||||||||||||
"T1" 12 months prior to beginning services |
"T2" Since Beginning Services (this year) |
If Suspended at T1 (Prior 12 Months) |
If Not Suspended at T1 (Prior 12 Months) |
Since starting to receive MH Services, the number of days my child was in school have |
|||||||||||||||||
# Suspended or Expelled |
# Not Suspended or Expelled |
No Response |
# Suspended or Expelled |
# Not Suspended or Expelled |
No Response |
# with an Expelled or Suspended in T2 |
# with No Suspension or Expulsion at T2 |
No Response |
# with an Expelled or Suspended in T2 |
# with No Suspension or Expulsion at T2 |
No Response |
# Greater (Improved) |
# Stayed the Same |
# Fewer days (gotten worse) |
# Not Applicable |
No response |
Total Responses |
|
|||
Total |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
||
Gender |
|
||||||||||||||||||||
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Gender NA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
Age |
|
||||||||||||||||||||
Under 18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
||
See Page 2 for additional Questions about the source of this data. |
|||||||||||||||||||||
Source of School Attendance Information 1) Consumer survey (recommended items) 2) Other Survey: Please send us items 3) Mental health MIS 4) State Education Department 5) Local Schools/Education Agencies 6) Other (specify) |
|||||||||||||||||||||
Measure of School Attendance 1) School Attendance 2) Other: (Specify) |
|
||||||||||||||||||||
Mental health programs include: ☐ 1) Children with SED only ☐ 2) Other Children (specify) ☐ 3) Both. |
|||||||||||||||||||||
Region for which data are reported: 1) The whole state 2) Less than the whole state (please describe) |
|
||||||||||||||||||||
What is the Total Number of Persons Surveyed or for whom School Attendance Data Are Reported Child/Adolescents |
|||||||||||||||||||||
1. If data is from a survey, what is the total number of people from which the sample was drawn? 2. What was your sample size? (How many individuals were selected for the sample)? 3. How many survey contacts were made? (surveys to valid phone numbers or addresses) 4. How many surveys were completed? (survey forms returned or calls completed) If data source was not a Survey, How many persons were data available for? 5. What was your response rate? (number of Completed surveys divided by number of Contacts): |
|
|
|||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
|
|||||||||||||||||||||
MHBG Table 23a (URS Table 20A) Profile of Non-Forensic (Voluntary and Civil-Involuntary) Patients Readmission to Any State Psychiatric Inpatient Hospital Within 30/180 Days of Discharge |
|||||
|
|
|
|||
|
|||||
MHBG Table 23a. |
|
||||
Report Year- From: To: |
|
|
|
|
|
State Identifier: |
|||||
|
Total number of Discharges in Year |
Number of Readmissions to ANY STATE Hospital within |
Percent Readmitted |
||
|
|
|
|
|
|
|
30 days |
180 days |
30 days |
180 days |
|
TOTAL |
0 |
0 |
0 |
|
|
Age |
|
|
|
|
|
0-12 |
|
|
|
|
|
13-17 |
|
|
|
|
|
18-20 |
|
|
|
|
|
21-64 |
|
|
|
|
|
65-74 |
|
|
|
|
|
75+ |
|
|
|
|
|
Not Available |
|
|
|
|
|
Gender |
|
|
|
|
|
Female |
|
|
|
|
|
Male |
|
|
|
|
|
Other |
|
|
|
|
|
Gender Not Available |
|
|
|
|
|
Race |
|
|
|
|
|
American Indian/ Alaska Native |
|
|
|
|
|
Asian |
|
|
|
|
|
Black/African American |
|
|
|
|
|
Hawaiian/Pacific Islander |
|
|
|
|
|
White |
|
|
|
|
|
|
|
|
|
|
|
More than one race |
|
|
|
|
|
Race Not Available |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Non-Hispanic/Latino |
|
|
|
|
|
Hispanic/Latino Origin Not Available |
|
|
|
|
|
Are Forensic Patients Included? |
|
|
|
|
|
Comments on Data: |
|||||
|
|
|
|
|
|
MHBG Table 23b (URS Table 20B) Profile of Forensic Patients Readmission to Any State Psychiatric Inpatient Hospital Within 30/180 Days of Discharge |
|||||
|
|
|
|||
MHBG Table 23b. |
|
||||
Report Year- From: To: |
|
|
|
|
|
State Identifier: |
|
|
|||
|
Total number of Discharges in Year |
Number of Readmissions to ANY STATE Hospital within |
Percent Readmitted |
||
|
|
|
|
|
|
|
|
30 days |
180 days |
30 days |
180 days |
TOTAL |
0 |
0 |
0 |
|
|
Age |
|
|
|
|
|
0-12 |
|
|
|
|
|
13-17 |
|
|
|
|
|
18-20 |
|
|
|
|
|
21-64 |
|
|
|
|
|
65-74 |
|
|
|
|
|
75+ |
|
|
|
|
|
Not Available |
|
|
|
|
|
Gender |
|
|
|
|
|
Female |
|
|
|
|
|
Male |
|
|
|
|
|
Other |
|
|
|
|
|
Gender Not Available |
|
|
|
|
|
Race |
|
|
|
|
|
American Indian/ Alaska Native |
|
|
|
|
|
Asian |
|
|
|
|
|
Black/African American |
|
|
|
|
|
Hawaiian/Pacific Islander |
|
|
|
|
|
White |
|
|
|
|
|
|
|
|
|
|
|
More than one race |
|
|
|
|
|
Race Not Available |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Non-Hispanic/Latino |
|
|
|
|
|
Hispanic/Latino Origin Not Available |
|
|
|
|
|
Comments on Data: |
|
|
|
|
|
|
|||||
MHBG Table 24 (URS Table 21) Profile of Non-Forensic (Voluntary and Civil-Involuntary Patients) Readmission to Any Psychiatric Inpatient Care Unit (State Operated or Other Psychiatric Inpatient Unit) Within 30/180 Days of Discharge |
|||||
|
|||||
MHBG Table 24 |
|
||||
Report Year- From: To: |
|
|
|
|
|
State Identifier: |
|||||
|
Total number of Discharges in Year |
Number of Readmissions to ANY Psychiatric Inpatient Care Unit Hospital within the state |
Percent Readmitted |
||
|
|
|
|
|
|
|
|
30 days |
180 days |
30 days |
180 days |
TOTAL |
0 |
0 |
0 |
|
|
Age |
|
|
|
|
|
0-12 |
|
|
|
|
|
13-17 |
|
|
|
|
|
18-20 |
|
|
|
|
|
21-64 |
|
|
|
|
|
65-74 |
|
|
|
|
|
75+ |
|
|
|
|
|
Not Available |
|
|
|
|
|
Gender |
|
|
|
|
|
Female |
|
|
|
|
|
Male |
|
|
|
|
|
Other |
|
|
|
|
|
Gender Not Available |
|
|
|
|
|
Race |
|
|
|
|
|
American Indian/ Alaska Native |
|
|
|
|
|
Asian |
|
|
|
|
|
Black/African American |
|
|
|
|
|
Hawaiian/Pacific Islander |
|
|
|
|
|
White |
|
|
|
|
|
|
|
|
|
|
|
More than one race |
|
|
|
|
|
Race Not Available |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Hispanic/Latino Origin |
|
|
|
|
|
Non-Hispanic/Latino |
|
|
|
|
|
Hispanic/Latino Origin Not Available |
|
|
|
|
|
1. Does this table include readmission from state psychiatric hospitals? |
|
|
|||
2. Are Forensic Patients Included? |
|
|
|
|
|
Comments on Data: |
|
||||
|
|||||
|
|||||
1Section 1915(b)(1) of the PHS Act (42 USC 300x-4).
2Section 1915(b)(2) of the PHS Act (42 USC 300x-4).
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Hartman, Jessica (SAMHSA) |
| File Modified | 0000-00-00 |
| File Created | 2022-10-03 |
© 2025 OMB.report | Privacy Policy