Form 1 Eligibility and Registration Form
Ambulatory Surgery Center Survey on Patient Safety Culture Database
Attachment A - ASC Eligibility and Registration Form
Eligibility and Registration Form
OMB: 0935-0242
AHRQ Ambulatory Surgery Center Survey on Patient Safety Culture Database, Supporting Statement A
Attachment A: Eligibility and Registration Form

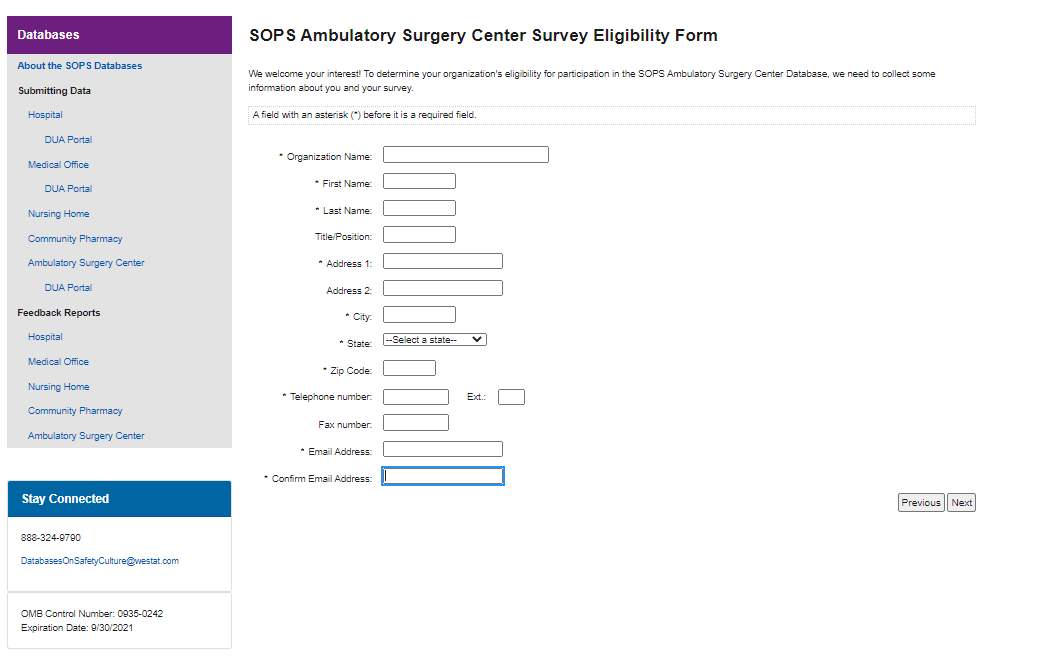
SOPS Ambulatory Surgery Center Survey Eligibility Form If the registration information is incorrect, please click on the "Previous" button below and update your information. Confirm your registration information Organization Name: Email: First Name: Last Name: Address 1: Address 2: City: State: Zip: Telephone: Fax: |
|


|

| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | Shakia Thornton |
| File Modified | 0000-00-00 |
| File Created | 2021-09-09 |
© 2026 OMB.report | Privacy Policy