Form 1 Attachment A FORM - MCH Block Grant Guidance_October_26_
Maternal and Child Health Services Block Grant Application/Annual Report Guidance
Attachment A FORM - MCH Block Grant Guidance_October_26_2020-FINAL
Application/Annual Report with Needs Assessment Summary
OMB: 0915-0172

TITLE V MATERNAL AND CHILD HEALTH SERVICES BLOCK GRANT TO STATES PROGRAM
GUIDANCE AND FORMS
FOR THE
TITLE V APPLICATION/ANNUAL REPORT
APPENDIX OF SUPPORTING DOCUMENTS
U.S. Department of Health and Human Services
Health Resources and Services Administration
Maternal and Child Health Bureau
Division of State and Community Health
Room 18N-33
5600 Fishers Lane, Rockville, MD 20857
(Phone 301-443-2204 FAX 301-443-9354)
TABLE of CONTENTS
APPENDIX A: HISTORY AND ADMNISTRATIVE BACKGROUND 1
APPENDIX B: PERFORMANCE MEASURE FRAMEWORK & IMPLEMENTATION 5
APPENDIX C: DETAIL SHEETS FOR THE NATIONAL OUTCOME MEASURES 24
AND NATIONAL PERFORMANCE MEASURES
APPENDIX D: FAMILY PARTNERSHIP 80
APPENDIX E: NEEDS ASSESSMENT – BACKGROUND AND CONCEPTUAL 81
FRAMEWORK
APPENDIX F: ASSURANCES AND CERTIFICATIONS 86
APPENDIX G: REQUIRED APPLICATION/ANNUAL REPORT COMPONENTS 89
AND TIMELINE
APPENDIX H: FINANCIAL BUDGET AND EXPENDITURE REPORTING 91
APPENDIX I: POPULATION HEALTH & CHILDREN WITH SPECIAL 97
HEALTH CARE NEEDS
APPENDIX J: MCH WORKFORCE CAPACITY 103
APPENDIX K: GLOSSARY 105
APPENDIX A: HISTORY AND ADMINISTRATIVE BACKGROUND
As one of the largest Federal block grant programs, Title V is a key source of support for promoting and improving the health of all the nation’s mothers and children. When Congress passed the Social Security Act in 1935, it contained the initial key landmark legislation which established Title V. This legislation is the origin of the federal government’s pledge of support to states and their efforts to extend and improve health and welfare services for mothers and children throughout the nation. To date, the Title V federal-state partnership continues to provide a dynamic program to improve the health of all mothers and children, including children with special health care needs (CSHCN).
The Maternal and Child Health Bureau
The Maternal and Child Health Bureau (MCHB) is the principal focus within Health Resources and Services Administration (HRSA) for all Maternal and Child Health (MCH) activities within the Department of Health and Human Services (HHS). MCHB’s mission is to improve the health of America’s mothers, children and families. We envision an America where all children and families are healthy and thriving. To achieve its mission, MCHB directs resources towards a combination of integrated public health services and coordinated systems of care for the MCH population.
Within the MCHB, the Division of State and Community Health (DSCH) has the administrative responsibility for the Title V MCH Services Block Grant to States Program (hereafter referred to as the MCH Block Grant). DSCH is committed to being the Bureau’s main line of communication with states and communities, in order to consult and work closely with both of these groups and others who have an interest in and contribute to the provision of a wide range of MCH programs and community-based service systems.
Maternal and Child Health Services Block Grant (Title V)
Under Title V, MCHB administers a Block Grant and competitive Discretionary Grants. The purpose of the MCH Block Grant is to create federal/state partnerships in 59 states and jurisdictions for developing service systems that address MCH challenges, such as:
• Significantly reducing infant mortality;
• Providing comprehensive care for all women before, during, and after pregnancy and childbirth;
• Providing preventive and primary care services for infants, children, and adolescents;
• Providing comprehensive care for children and adolescents with special health care needs;
• Immunizing all children;
• Reducing adolescent pregnancy;
• Preventing injury and violence;
• Putting into community practice national standards and guidelines for prenatal care, for healthy and safe childcare, and for the health supervision of infants, children, and adolescents;
• Assuring access to care for all mothers and children; and
• Meeting the nutritional and developmental needs of mothers, children and families.
Under Title V, MCHB also administers two types of Federal Discretionary Grants, Special Projects of Regional and National Significance (SPRANS) and Community Integrated Service Systems (CISS) grants. SPRANS funds projects (through grants, contracts, and other mechanisms) in research, training, genetic services and newborn screening/follow-up, sickle cell disease, hemophilia, and MCH improvement. CISS projects (through grants, contracts, and other mechanisms) seek to increase the capacity for service delivery at the local level and to foster formation of comprehensive, integrated, community level service systems for mothers and children.
In addition to SPRANS and CISS grants, the MCHB also administers the following categorical programs:
• Emergency Medical Services for Children;
• Sickle Cell Disease Treatment Demonstration Program;
• Healthy Start Initiative;
• Universal Newborn Hearing Screening;
Heritable Disorder Program;
• Autism;
• Maternal, Infant, and Early Childhood Home Visiting Program; and
Family to Family Health Information Centers.
In recent years, some state Title V programs have begun to utilize the life course model as an organizing framework for addressing identified MCH needs. The life course approach points to broad social, economic, and environmental factors as underlying contributors to health and social outcomes. This approach also focuses on persistent inequalities in the health and well-being of individuals and how the interplay of risk and protective factors at critical points of time can influence an individual’s health across his/her lifespan and potentially across generations.
Maternal and Child Health Block Grant (State Formula Grants)
Since its original authorization in 1935, Title V of the Social Security Act has been amended several times to reflect the increasing national interest in maternal and child health and well-being. One of the first changes occurred when Title V was converted to a block grant program as part of the Omnibus Budget Reconciliation Act (OBRA) of 1981. This change resulted in the consolidation of seven categorical programs into a single block grant. These programs included:
Maternal and Child Health and Services for Children with Special Health Care Needs;
Supplemental Security Income for children with disabilities;
Lead-based paint poisoning prevention programs;
Genetic disease programs;
Sudden infant death syndrome programs;
Hemophilia treatment centers; and
Adolescent pregnancy grants.
Another significant change in the Title V MCH Block Grant came as a result of the Omnibus Budget Reconciliation Act (OBRA) of 1989, which specified new requirements for accountability. The amendments enacted under OBRA introduced stricter requirements for the use of federal funds and for state planning and reporting. Congress sought to balance the flexibility of the block grant with greater accountability, by requiring State Title V programs to report their progress on key MCH indicators and other program information. Thus, the block grant legislation emphasizes accountability while providing states with appropriate flexibility to respond to state-specific MCH needs and to develop targeted interventions and solutions for addressing them. This theme of assisting states in the design and implementation of MCH programs to meet state and local needs, while at the same time asking them to account for the use of federal/state Title V funds, was embodied in the requirements contained in the Guidance documents for the state MCH Block Grant Applications/Annual Reports.
In 1993 the Government Performance and Results Act (GPRA), Public Law 103-62, required federal agencies to establish measurable goals that could be reported as part of the budgetary process. For the first time, funding decisions were linked directly with performance. Among its purposes, GPRA is intended to “...improve Federal program effectiveness and public accountability by promoting a new focus on results, service quality, and customer satisfaction.” GPRA requires each federal agency to develop comprehensive strategic plans, annual performance plans with measurable goals and objectives, and annual reports on actual performance compared to performance goals. The MCHB effort to respond to GPRA requirements coincided with other planned improvements to the MCH Block Grant Guidance. As a result, the MCH Block Grant Application/Annual Report and forms contained in the 1997 edition of the Maternal and Child Health Services Title V Block Grant Program - Guidance and Forms for the Title V Application/Annual Report served to ensure that the states and jurisdictions could clearly, concisely, and accurately tell their MCH “stories.” This Application/Annual Report became the basis by which MCHB met its GPRA reporting requirements for the MCH Block Grant to States Program.
In 1996, the MCHB began a process of programmatic assessments and planning activities aimed at improving the Title V MCH Block Grant Application/Annual Report Guidance document for states. Since that time, the Maternal and Child Health Services Title V Block Grant Program - Guidance and Forms for the Title V Application/Annual Report (Guidance) has been revised eight times. Updated Guidance documents are submitted to and approved by the Office of Management and Budget (OMB) prior to their release. Revisions to each subsequent edition of the Guidance have considered changes in MCH priorities, availability of new national data sources and opportunities for refining and streamlining the Application/Annual Report preparation and submission process for states. The reduced burden that resulted from this latter commitment was largely achieved through efficiencies that were created by the electronic reporting vehicle for the state MCH Block Grant Applications/Annual Reports, specifically the Title V Information System (TVIS.)
Title V Information System
The development of an electronic reporting package in 1996 was a significant milestone for the State MCH Block Grants. Advances in technology allowed for the development of a web based Title V Information System (TVIS). The TVIS is designed to capture the performance data and other program and financial information contained in the state Applications/Annual Reports. While descriptive information is available on state Title V-supported efforts, state MCH partnership efforts and other program-specific initiatives of the state in meeting its MCH needs, TVIS primarily serves as an online, Web-accessible interface for the submission of the 59 state and jurisdictional Title V MCH Block Grant Applications/Annual Reports each year by July 15th. Developed in conjunction with the program requirements outlined in the Title V MCH Block Grant Application/Annual Report Guidance, the TVIS is available to the public on the World Wide Web at: https://mchb.tvisdata.hrsa.gov/. Over the years, the TVIS has increasingly become recognized as a powerful and useful tool for a number of audiences. The “transformation” of the State MCH Block Grant program in 2015 mandated the development of a new data collection and web report system for the TVIS. HRSA continues to provide funding support for a contract to develop, maintain and enhance the TVIS annually.
Integrated with HRSA’s grants management system (i.e., the HRSA Electronic Handbooks (EHB),) the TVIS makes available to the public through its web reports the key financial, program, performance, and health indicator data reported by states in their yearly MCH Block Grant Applications/Annual Reports. Examples of the data that are collected include: information on populations served; budget and expenditure breakdowns by source of funding, service and program; program data, such as individuals served and breakdowns of MCH populations; other state data (OSD); and performance and outcome measure data for the national and state measures. Reporting on performance relative to the national measures is used to assess national progress in key MCH priority areas and to facilitate the Bureau’s annual GPRA reporting.
APPENDIX B: |
PERFORMANCE MEASURE FRAMEWORK & IMPLEMENTATION
|
Overview of the Framework
The national performance measure framework is based on a three-tiered performance measure system: National Outcome Measures (NOMs), National Performance Measures (NPMs), and Evidence-based or -informed Strategy Measures (ESMs). In brief, NOMs are the ultimate health outcomes that Title V is attempting to improve. The NPMs are considered to be more directly modifiable by state Title V program efforts and influence NOMs. ESMs are developed by states to capture their evidence-based or -informed programmatic efforts to affect NPMs and in turn NOMs. The framework is intended to highlight the impact of Title V investments and provides states with flexibility in selecting NPMs and developing state performance measures (SPMs) and ESMs to address the state’s priority needs. The minimum number of required NPM selections is five. There needs to be at least one NPM in each of the five population domains. States may select as many NPMs and SPMs as needed to reflect priority needs identified from the five-year needs assessment.
Title V Performance Measure Framework
Evaluation Logic Model

In the above figure, which compares the Title V performance measure framework to an evaluation logic model, measures were designated as NOMs, which primarily reflect longer-term indicators of population health status, if they met one or more of the following criteria: the measure was mandated by the Title V legislation that the data be collected (Table 1), even if not a long-term indicator; it was considered a sentinel health marker for women, infants, or children; it was a major focus of either the Title V legislation or Title V activities; it was considered an important health condition to monitor because the prevalence was increasing, but the reasons for the increase were unclear; or there was a recognized need to move the MCH field forward in this area, even if there was not yet a consensus on how to measure the construct. The latter were considered developmental outcome measures. There are 25 NOMs, of which 4 have additional sub-measures.
Table 1. Measures mandated by Title V legislation1
Measure |
Related NOMs |
Rate of Infant Mortality |
NOM 9.1 |
Rate of Low Birth Weight Births |
NOM 4 |
Rate of Maternal Mortality |
NOM 3 |
Rate of Neonatal Death |
NOM 9.2 |
Rate of Perinatal Death |
NOM 8 |
Number of children with chronic illness and the type of illness |
NOMs 17.1-17.4 |
Proportion of infants born with fetal alcohol syndrome2 |
NOM 10 |
Proportion of infants born with drug dependency |
NOM 11 |
Proportion of women who do not receive prenatal care during the first trimester of pregnancy |
NOM 1 |
Proportion of children by age 2 vaccinated against measles, mumps, rubella, polio, diphtheria, tetanus, pertussis, Hib meningitis, and hepatitis B |
NOM 22.1 |
1Sec. 506(a)(2)(B) of the Social Security Act [42 U.S.C. 706 (a)(2)(B)] https://www.ssa.gov/OP_Home/ssact/title05/0506.htm
2Operationalized as “percent of women who drink alcohol in the last 3 months of pregnancy” due to a lack of available data on FASD prevalence.
Measures
were considered as NPMs, or short or medium term indicators of health
behaviors or health care access/quality, if they met one or more of
the following criteria: there was a large investment of resources as
determined by the state narratives; the measure was considered
modifiable through Title V activities; a state could delineate
measurable activities to address the performance measure; significant
disparities existed among population groups; research had indicated
that the condition or activity had large societal costs; or research
had indicated that the promotion of certain behaviors, practices or
policies had improved outcomes. There also had to be evidence that
an NPM was associated with at least one of the NOMs (see Table 3 in
this Appendix) for evidence-based or -informed linkages between NPMs
and NOMs). However, it is important to recognize that NOMs are
multifactorial and improvement in a given NPM may not necessarily
result in improvement of the associated NOM. Fifteen NPMs were
identified for the Title V MCH Services Block Grant.
The ESMs are the key to understanding how a state Title V program tracks programmatic investments or inputs designed to impact the NPMs. In the framework, states select evidence-based or evidence-informed strategies and activities designed to impact the NPMs; states then create ESMs to track state Title V strategies contained in the State Action Plan. The development of ESMs is guided through an examination of evidenced-based or -informed strategies, and determining what components are practical, meaningful, measurable, and moveable. The main criteria for ESMs are being meaningfully related to the selected NPM through scientific evidence or theory and being measurable by the state with improvement achievable in multiple years of the five-year reporting cycle. (The Guidance for Implementation of Performance Measurement Framework section below provides more detailed information on ESMs.)
The 15 NPMs address key national MCH priority areas in five MCH population health domains: 1) Women/Maternal Health; 2) Perinatal/Infant Health; 3) Child Health; 4) Adolescent Health; and 5) CSHCN. The five MCH population health domains are contained within the three legislatively-defined MCH populations [Section 505(a)(1).] The first two domains are included under “preventive and primary care services for pregnant women, mothers and infants up to age one,” which is the first of the three defined MCH populations. The third and fourth domains, child and adolescent health, are included in the second defined MCH population, specifically “preventive and primary care services for children.” Services for CSHCN is the third legislatively-defined MCH population. Presented in the table below are the 15 NPMs and the corresponding MCH Population domain(s) and applicable subgroup options for ESMs.
Table 2. NPMs and MCH Population Domains
NPM # |
National Performance Measures |
MCH Population Domains |
ESM Subgroup Options (if applicable) |
1 |
Well-woman visit |
Women/Maternal Health |
|
2 |
Low-risk cesarean delivery |
Women/Maternal Health |
|
3 |
Risk-appropriate perinatal care |
Perinatal/Infant Health |
|
4 |
Breastfeeding |
Perinatal/Infant Health |
|
5 |
Safe sleep |
Perinatal/Infant Health |
|
6 |
Developmental screening |
Child Health |
|
7 |
Injury hospitalization |
Child Health and/or Adolescent Health |
Children 0 through 9 Adolescents 10 through 19 All Children 0 through 19 |
8 |
Physical activity |
Child Health and/or Adolescent Health |
Children 6 through 11 Adolescents 12 through 17 All Children 6 through 17 |
9 |
Bullying |
Adolescent Health |
|
10 |
Adolescent well-visit |
Adolescent Health |
|
11 |
Medical home |
Children with Special Health Care Needs (CSHCN), Child and Adolescent Health |
CSHCN CSHCN and non-CSHCN |
12 |
Transition |
Children with Special Health Care Needs (CSHCN) and Adolescent Health |
CSHCN CSHCN and non-CSHCN |
13 |
Preventive dental visit – Pregnancy Preventive dental visit – Child/Adolescent |
Women/Maternal Health, Child Health, and/or Adolescent Health |
Pregnant women Children 0 through 5 Children 6 through 11 Adolescents 12 through 17 All Children 0 through 17 |
14 |
Smoking – Pregnancy Smoking – Household |
Women/Maternal Health, Child Health, and/or Adolescent Health |
Pregnant women Children 0 through 5 Children 6 through 11 Adolescents 12 through 17 All Children 0 through 17 |
15 |
Adequate insurance |
Child Health, Adolescent Health, and/or Children with Special Health Care Needs (CSHCN) |
All Children CSHCN |
The NPMs incorporate two significant concepts: first, Title V is responsible for promoting the health of all mothers and children, which includes an emphasis on CSHCN and their families; and second, the development of life course theory has indicated that there are critical stages, beginning before a child is born and continuing throughout life, which can influence lifelong health and wellbeing (see Table 4 in this Appendix for a crosswalk of NPM/NOMs and AMCHP Lifecourse Indicators).
A sixth domain, Cross-Cutting/Systems Building, allows states to focus on public health system issues that impact all MCH population groups. This domain does not contain any NPMs but allows states to develop unique SPMs to address priority areas that cut across all population health domains. Example SPM topics may include but are not limited to:
Family partnership activities across all population health domains;
Social determinants of health;
Health equity;
Workforce development; and
Enhancement of data infrastructure.
Implementation of Measurement
National Outcome Measures
NOMs are longer-term and/or legislatively required indicators, many of which may be influenced by NPMs (see Table 3) and are important to monitor and assess as a core function of public health that may stimulate program and policy action. Thus, NOMs should be tracked to understand the MCH population’s health, and are important for the development of the needs assessment and selection of NPMs. Changes in NOM indicators, which may result from improvement in NPMs, can be discussed in the appropriate population domain section of the narrative, but there is not a reporting requirement for this discussion. Data for NOMs will be prepopulated, where possible. States do not provide performance objectives for NOMs.
National Performance Measures
In implementing this framework, states will choose a minimum five out of 15 NPMs for its Title V program to address during the current five-year needs assessment cycle, at least one in each MCH population domain. When selecting NPMs, it is important that the alignment of the NPMs to the state identified priorities is clear. If the priority does not align with a NPM, the state should develop a state performance measure (SPM). When selecting NPM #4 or NPM #5, all sub-measures are included as part of the NPM and individual sub-measures cannot be selected as the NPM in TVIS. To promote flexibility, each MCH population domain contains at least three NPM options. There are no mandatory NPMs and no maximum for the number of NPMs that a state can select. The same measure selected in multiple domains (NPM #7, NPM #8, NPM #11, NPM #12, NPM #13, NPM #14 and NPM #15) will only count once toward the minimum of five.
For example, if a state selects a compound measure such as NPM #14 in Women/Maternal Health and Child Health, it would only count once towards the minimum of five NPMs, and another measure would need to be selected in either Women/Maternal or Child Health to satisfy the requirement of one measure in each population domain. Injury hospitalization, physical activity, medical home, preventive dental visit, household smoking, and adequate insurance can be selected for either the Child or the Adolescent Health domains, or both, because the age ranges span both domains. It is recognized that the strategies and accompanying ESMs may be different, depending on the children’s ages, for injury hospitalization, physical activity, preventive dental visit, and household smoking; therefore, these measures have various subgroup options for specifying the focus of ESMs. Given their particular importance for CSHCN, medical home and transition must include a focus on CSHCN, even if they are selected within the Child and/or Adolescent Health domain.
In
the last reporting year of the previous Guidance that expired on
12/31/2020, states selected a minimum of five NPMs to complete in
the new five-year needs assessment cycle (2021-2025).
States
will continue to report 2019 and 2020 indicator data for NPMs from
the previous needs assessment cycle (2016-2020) that they chose to
not continue into the new cycle.
Once NPMs are
selected, a state will track the five NPMs throughout the five-year
reporting cycle. States are encouraged not to change the selected
NPMs during the five-year reporting cycle. This
Guidance covers years 2-4 of the current five-year reporting cycle.
States are encouraged to continue using measures selected in the FY
2021 application (year 1 of the five-year reporting cycle). If
a state determines that a NPM needs to be changed or retired, clear
justification must be provided. In an effort to reduce state burden,
annual performance data (indicator/numerator/ denominator) for the
NOMs and the NPMs will be prepopulated by MCHB from national data
sources, as available, and provided to the states for their use in
preparing the yearly Title V MCH Services Block Grant
Applications/Annual Reports. Data will be provided overall by year
to facilitate objective-setting and performance monitoring, as well
as by various demographic stratifiers (e.g., age, race/ethnicity,
education, urban/rural residence) to identify priority populations
for targeting strategies and programmatic interventions. Performance
objectives for future years can be changed for individual NPMs based
on ongoing needs assessment efforts and performance monitoring.
![]()
![Lol_exclam[1].png](106167900_html_c9b1776d4b10db3f.gif)
States also have the opportunity to develop SPMs that will specifically impact infrastructure through the Cross-cutting/Systems Building domain to improve the areas impacting multiple population domains like family partnership and data infrastructure.
When selecting new measures it is important that the following checklist items have been satisfied.
Measure Checklist |
Check if Answer is Yes |
A minimum of 5 NPMs is selected |
□ |
There is at least one NPM selected for each population health domain
*NPM #7, #8, #11, #12, #13, #14, #15 selected in multiple domains count once toward the minimum of five |
□ |
There is a NPM/SPM for each state priority |
□ |
All selected NPMs/SPMs have clear alignment with the state priorities |
□ |
Additional guidance on use of provisional data for NPMs, lack of a national data source for NPMs, and use of integrated measures is provided below:
Use of Provisional Data: States may, but are not required to, include more timely provisional data if they choose. Providing this data will not replace the prepopulated final data provided for the measures.
Lacking a National Data Source: States can choose a measure if they do not have the data source noted on the detail sheet, as long as they provide the indicator, numerator and denominator data as defined on the detail sheet (Appendix C). For Pregnancy Risk Assessment Monitoring System (PRAMS), states will be able to submit their PRAMS or PRAMS-like data to TVIS following the same definition for a given measure if CDC cannot furnish it. The same situation may apply to other data sources. If a state provides its own data from a different source, this should be annotated in a field note. If a state cannot provide data for a given measure with the same definition as listed on the detail sheet, the state should consider creating a SPM.
Integrated Measures (NPM #13 and NPM #14): The integrated measures of preventive dental visit and smoking have two distinct measures, one in pregnancy and one for children/adolescents. States may select these NPMs for one or more of the following MCH population domains: Women/Maternal Health; Child Health; Adolescent Health. If a state selects one of these NPMs for Women/Maternal Health (#13.1 and NPM #14.1) and also for Child and/or Adolescent Health (NPM #13.2 and NPM #14.2), states will be expected to develop multiple ESMs, at least one for each measure.
Evidence-based or -informed Strategy Measures
For each selected NPM, states must develop at least one ESM to quantify and assess the outputs of the identified State Title V strategies that are linked to each selected NPM. The main steps for developing ESMs include 1) review the evidence base for effective strategies, 2) operationalize outputs of strategy as a measure and, 3) set improvement objectives that are achievable over multiple years or throughout the five-year reporting cycle.
When
developing ESMs, remember to: Review
the evidence base
– Your state should start by choosing evidence-based or
–informed strategies that are known to impact your state’s
selected NPMs. Operationalize
outputs of your chosen strategies
– Quantifying outputs (e.g., number, percent and rate) will
allow your state will show measurable improvement over time. Set
objectives for improvement
– This provides an important check to make sure improvement
is possible and attainable.
States are only required to have at least one
active ESM for each of the NPMs selected. Most issues in MCH are
multifactorial, therefore, states are encouraged to develop multiple
strategies, each with a related ESM, to impact a selected NPM. Given
that ESMs capture state programmatic efforts, it is recommended that
states develop corresponding ESMs for strategies in which they are
investing the most activity and/or funding.
Steps for Developing ESMs:
Review the evidence base for effective strategies: This step requires a review of the evidence to select strategies that are meaningfully related to the NPMs through scientific evidence or theory. The key for selecting an effective strategy to impact an NPM is identifying evidence-based or – informed practices. Evidence-based strategies are those that have either moderate evidence or are scientifically rigorous, while evidence-informed are those that have emerging evidence or are based on expert opinion. “Evidence-informed” is meant to convey that there is information suggesting that a certain strategy could be effective in addressing a NPM. These are strategies that have not yet been rigorously tested or evaluated but that incorporate a theoretical model from other effective public health practices or apply a novel approach grounded in scientific theory. For more information on this continuum and its rationale, review the Evidence Ratings model, adapted from the Robert Wood Johnson What Works for Health project (https://www.mchevidence.org/tools/).
Beyond scientific evidence of effectiveness, additional considerations of reach, feasibility, sustainability, and transferability should be considered in terms of likely impact. It is important to note that there may be a need for states to adapt strategies based on differences in populations and settings, available resources and other considerations. A given strategy should be based on, or informed by, evidence of effective practice in direct relation to improving the NPM rather than a strategy that has an indirect relationship. An example of an indirect relationship may include efforts to improve the content or quality of well-woman or adolescent visits as a strategy for improving access or utilization. While the ESMs may be either directly or indirectly related to the NPM, states/jurisdictions are encouraged to select at least one ESM that directly corresponds to the selected NPM. The strategy should be relevant to state priorities and tailored or adapted for contextual settings and population groups where applicable. It is critical for the strategy to be feasible for the state to implement within the five-year cycle and involve stakeholder input or buy-in from partners who may be instrumental in successfully executing the strategy or tracking output. The strategy should also have potential for improvement (i.e., not already or nearly accomplished).
Operationalize the outputs of the strategy as a measure: Once the state identifies a strategy it intends to use, the state will develop and operationalize the outputs of this strategy as a measure or ESM. Given that ESMs are intended to measure progress over time, they should be quantifiable (e.g., number, percent, rate, count), well-defined and specific (i.e., specifically defined indicator, numerator, and denominator), and there should be data available to measure and track the ESM with incremental change over time.
Set improvement objectives that are achievable: The setting of improvement objectives offers an important check that improvement in the ESM is expected and attainable over multiple assessments within a reasonable time period. Objectives should reflect an improvement goal over multiple years of the five-year reporting cycle rather than a static objective over time.
The checklist below may be helpful in identifying a meaningful strategy and operationalizing the output as a measure.
ESM Checklist |
Check if Answer is Yes |
1: The strategy is meaningful |
|
The strategy is evidence-based/informed in direct relation to the NPM |
□ |
The strategy is relevant to state priorities and context |
□ |
The strategy is feasible and involved stakeholder input or buy-in |
□ |
The strategy has potential for improvement |
□ |
2: The strategy output is measurable as an ESM |
|
The ESM is a number, %, rate, count, yes/no* |
□ |
The ESM is well-defined and specific |
□ |
Data are available to measure and track the ESM over time with multiple assessments |
□ |
3: The ESM is moveable |
|
Improvement in the ESM is attainable within the 5-year needs assessment and reporting cycle |
□ |
The ESM can show incremental change over time |
□ |
*Quantitative measures are recommended over qualitative yes/no measures to quantify strategy outputs and show incremental improvement over time in relation to the NPM.
States should work closely with family partnerships as they revise and develop the ESMs for their selected NPMs. For the Title V MCH Services Block Grant, family partnership is defined as patients, families, their representatives, and health professionals working in active partnership at various levels across the health care system - direct care, organizational design, governance and policy making - to improve health and health care. 2 This partnership is accomplished through the intentional practice of working with families for the ultimate goal of positive outcomes in all areas through the life course.
Development of Detail Sheets for ESMs
As a new ESMs are introduced, a state will develop a detail sheet for each ESM, which it will submit as part of its Application/Annual Report. On the detail sheet, the state will define the: (1) measure; (2) linkage to broader framework; (3) description of evidence-based/informed strategy; (4) goal; (5) significance; (6) indicator, numerator, denominator; and (7) data source and data issues.
A Note on Count Measures – Adding a
denominator Count
measures (e.g., # providers trained) are not bad in and of
themselves and are preferable to qualitative yes/no measures to
capture the impact of a strategy. For example, it is important to
know that 200 providers received training. A count alone will not
measure the full coverage or reach of a strategy within a state. If
there are 200 providers in the state, then 100% were reached. If
there are 20,000 providers, only 1% were reached. By adding a
denominator and making the count a percentage, it is possible to
track progress relative to the actual need within a state and
understand when the strategy objective has been achieved.
Tracking of ESMs
States will track performance for the ESMs that were established for this five-year needs assessment cycle. States will determine performance objectives for each of the ESMs in the application year. These objectives can be revised, as needed, for future reporting years. Data for the ESMs (i.e., numerator/denominator) will be entered annually by the state. During the five-year reporting cycle, ESMs may be added, modified, replaced, or retired, as new strategies or measurement methods emerge, objectives are achieved without further room for improvement, or the strategy did not produce intended results.
State Performance and Outcome Measures
To
address state priorities not addressed by the National Performance
Measures, the State Performance Measures (SPMs) can be developed.
Similarly,
if the definition of the NPM does not align with the priority, the
state should develop a related SPM. For example, if the priority is
only focused on one sub-measure of an NPM such as NPM #4 or NPM #5,
then that sub-measure should be created as an SPM. There
is no minimum or maximum number of SPMs required. The combination of
NPMs with state-developed SPMs allows the state flexibility to
reflect its priority needs from the most recent Five-Year Needs
Assessment. For the developed SPMs, the state will continue with the
performance objectives for five years (FY 2021-FY 2025) for each of
the measures. A state may revise its SPM objectives in future years’
Applications/Annual Reports. The development of the SPMs coincides
with the selection of NPMs and the development of the state ESMs.
A state will develop a detail sheet for each of these measures, which will define the:
(1) measure; (2) goal; (3) indicator, numerator, and denominator; (4) data source; and
(5) significance. States will track their developed SPMs throughout the five-year reporting cycle. Data for the SPMs (i.e., indicator/numerator/denominator) will be entered annually by the state. A state can retire a SPM during the five-year reporting cycle and replace it with another SPM based on its MCH priority needs. A state is not required to develop ESMs for SPMs.
A state may also develop, if it chooses, one or more State Outcome Measures (SOMs) based on its MCH priorities, as determined by the findings of the Five-Year Needs Assessment, provided that none of the NOMs address the same priority area for the state. An SOM should be linked with a performance measure to show the impact of performance on the intended outcome. States will track the SOMs during the five-year reporting cycle and the SOM can be retired if the state chooses. Data for the SOMs (i.e., indicator/numerator/ denominator) will be entered annually by the state.
Available Resources
MCH Library
The Maternal and Child Health (MCH) Digital Library provides access to current evidence to support State Title V programs, community agencies, educators, students, researchers, policymakers, and families. The library also provides access to seminal and historic materials from federal, state, and local programs. The overarching goal of the library is to serve the MCH community with accurate, reliable, and timely information and resources.
Strengthening the Evidence Base for Maternal and Child Health Programs https://www.mchevidence.org/
This is a consortium-based project bringing multiple partners together including the National Center for Education in Maternal and Child Health, National Maternal and Child Workforce Development Center, CityMatCH, AMCHP, and the Georgetown University Center for Child and Human Development. The purpose of the project is to provide expert consultation, technical assistance (TA), and resources to assist state Title V MCH Block Grant programs in developing evidence based-/informed State Action Plans and strategies that advance National Performance Measures (NPMs). In addition to individual TA-requests, the MCH Evidence website provides a variety of resources to help states review evidence-based or -informed strategies and develop evidence-based or –informed strategy measures (ESMs) for each National Performance Measure.
Innovation Station
http://www.amchp.org/programsandtopics/BestPractices/InnovationStation/Pages/Innovation-Station.aspx
AMCHP’s Innovation Station is a collection of best practices and innovative strategies developed and submitted by State Title V agencies to facilitate state-to-state sharing. In addition to searching for best practices by NPM, states are able to access implementation guides, apply for funding to replicate best practices, and request technical assistance. States are invited to participate by submitting best practices or joining a MCH Population Community of Practice (CoP).
Table 3. Evidence-based/informed National Performance and Outcome Measure Linkages*
National Outcome Measure |
National Performance Measure |
|||||||||||||||
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
||
# |
Short Title |
Well-woman visit |
Low-risk cesarean delivery |
Risk-appropriate perinatal care |
Breastfeeding |
Safe sleep |
Developmental screening |
Injury hospitalization |
Physical activity |
Bullying |
Adolescent well-visit |
Medical home |
Transition |
Preventive dental visit |
Smoking |
Adequate insurance |
1 |
Early prenatal care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
Severe maternal morbidity |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
X |
|
3 |
Maternal mortality |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
X |
|
4 |
Low birth weight |
X |
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
5 |
Preterm birth |
X |
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
6 |
Early term birth |
X |
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
7 |
Early elective delivery |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
Perinatal mortality |
X |
|
X |
|
|
|
|
|
|
|
|
|
|
X |
|
9.1 |
Infant mortality |
X |
|
X |
X |
X |
|
|
|
|
|
|
|
|
X |
|
9.2 |
Neonatal mortality |
X |
|
X |
|
|
|
|
|
|
|
|
|
|
X |
|
9.3 |
Postneonatal mortality |
X |
|
|
X |
X |
|
|
|
|
|
|
|
|
X |
|
9.4 |
Preterm-related mortality |
X |
|
X |
|
|
|
|
|
|
|
|
|
|
X |
|
9.5 |
SUID mortality |
|
|
|
X |
X |
|
|
|
|
|
|
|
|
X |
|
10 |
Drinking during pregnancy |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
Neonatal abstinence syndrome |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
Newborn screening timely follow-up |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
School readiness |
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
14 |
Tooth decay/cavities |
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
15 |
Child mortality |
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
16.1 |
Adolescent mortality |
|
|
|
|
|
|
X |
|
X |
X |
|
|
|
|
|
16.2 |
Adolescent motor vehicle death |
|
|
|
|
|
|
X |
|
|
X |
|
|
|
|
|
16.3 |
Adolescent suicide |
|
|
|
|
|
|
X |
|
X |
X |
|
|
|
|
|
17.1 |
CSHCN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17.2 |
CSHCN systems of care |
|
|
|
|
|
|
|
|
|
X |
X |
X |
X |
|
X |
17.3 |
Autism |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17.4 |
ADD/ADHD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18 |
Mental health treatment |
|
|
|
|
|
|
|
|
|
X |
X |
|
|
|
X |
19 |
Overall health status |
|
|
|
|
|
X |
|
X |
|
X |
X |
|
X |
X |
X |
20 |
Obesity |
|
|
|
|
|
|
|
X |
|
X |
|
|
|
|
|
21 |
Uninsured |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22.1 |
Child vaccination |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
22.2 |
Flu vaccination |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
X |
22.3 |
HPV vaccination |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
X |
22.4 |
Tdap vaccination |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
X |
22.5 |
Meningitis vaccination |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
X |
23 |
Teen births |
X |
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
24 |
Postpartum depression |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25 |
Forgone health care |
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
X |
* Includes linkages based on expert opinion or theory in the absence of empirical scientific evidence. Associations with available empirical scientific evidence that is mixed or inconclusive are not included. This table is subject to revision as new scientific evidence becomes available. By definition, NPMs must be linked to at least one NOM; however, not all NOMs must have linked NPMs, as they may be important to monitor as sentinel health indicators regardless.
References for Table 3
NPM-1 Well-Woman Visit
Johnson K. Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, Boulet S, Curtis MG. Recommendations to Improve Preconception Health and Health Care—United States: A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep. 2006 Apr 21;55(RR-6):1-23. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5506a1.htm
Moos MK, Dunlop AL, Jack BW, Nelson L, Coonrod DV, Long R, Boggess K, Gardiner PM. Healthier women, healthier reproductive outcomes: recommendations for the routine care of all women of reproductive age. Am J Obstet Gynecol. 2008 Dec;199(6 Suppl 2):S280-9. https://www.ajog.org/article/S0002-9378(08)01029-6/fulltext
NPM-2 Low-Risk Cesarean Delivery
Safe prevention of the primary cesarean delivery. Obstetric Care Consensus No. 1. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:693–711. http://www.acog.org/Resources-And-Publications/Obstetric-Care-Consensus-Series/Safe-Prevention-of-the-Primary-Cesarean-Delivery
NPM-3 Risk-Appropriate Perinatal Care
American Academy of Pediatrics Committee on Fetus And Newborn. Levels of neonatal care. Pediatrics. 2012 Sep;130(3):587-97. http://pediatrics.aappublications.org/content/130/3/587
NPM-4 Breastfeeding
Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC; Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016 Jan 30;387(10017):475-90. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)01024-7/fulltext
American Academy of Pediatrics Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 2012 Mar;129(3):e827-41. http://pediatrics.aappublications.org/content/early/2012/02/22/peds.2011-3552
Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012 Aug 15;(8):CD003517. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003517.pub2/full
Ip S, Chung M, Raman G, Chew P, Magula N, DeVine D, Trikalinos T, Lau J. Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries. Evid Rep Technol Assess (Full Rep). 2007 Apr;(153):1-186. https://www.ncbi.nlm.nih.gov/books/NBK38337/
NPM-5 Safe Sleep
Taskforce on Sudden Infant Death Syndrome. SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping Environment. Pediatrics. 2016 Nov;138(5). http://pediatrics.aappublications.org/content/138/5/e20162938
Moon RY, Taskforce on Sudden Infant Death Syndrome. SIDS and Other Sleep-Related Infant Deaths: Evidence Base for 2016 Updated Recommendations for a Safe Infant Sleeping Environment. Pediatrics. 2016 Nov;138(5). https://pediatrics.aappublications.org/content/138/5/e20162940
NPM-6 Developmental Screening
Council on Children With Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children With Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics. 2006 Jul;118(1):405-20. http://pediatrics.aappublications.org/content/118/1/405
Hagan, JF, Shaw JS, Duncan PM. Bright Futures: guidelines for health supervision of infants, children and adolescents. Fourth Edition. Elk Grove Village, IL: American Academy of Pediatrics. 2017.
NPM-7 Injury Hospitalization
Centers for Disease Control and Prevention (CDC). VitalSigns: Child Injury. April 2012. https://www.cdc.gov/vitalsigns/childinjury/
Centers for Disease Control and Prevention (CDC). Suicide: Facts at a Glance. https://www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf
Centers for Disease Control and Prevention (CDC). Youth Violence: Facts at a Glance. https://www.cdc.gov/violenceprevention/pdf/yv-datasheet.pdf
NPM-8 Physical Activity
U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd Edition. 2018. https://health.gov/our-work/physical-activity/current-guidelines
NPM-9 Bullying
Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, Wolfe M, Reid G. Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics. 2015 Feb;135(2):e496-509. http://pediatrics.aappublications.org/content/135/2/e496
NPM-10 Adolescent Well-Visit
National Adolescent and Young Adult Health Information Center (2016). Summary of Recommended Guidelines for Clinical Preventive Services for Adolescents up to age 18. San Francisco, CA: National Adolescent and Young Adult Health Information Center, University of California, San Francisco. Retrieved from http://nahic.ucsf.edu/adolescent-guidelines
Adams SH, Park MJ, Twietmeyer L, Brindis CD, Irwin CE. Increasing Delivery of Preventive Services to Adolescents and Young Adults: Does the Preventive Visit Help? J Adolesc Health. 2018 Aug;63(2):166-171. doi: 10.1016/j.jadohealth.2018.03.013. Epub 2018 Jun 19. https://www.sciencedirect.com/science/article/abs/pii/S1054139X1830137X
NPM-11 Medical Home
Hadland SE, Long WE. A systematic review of the medical home for children without special health care needs. Matern Child Health J. 2014 May;18(4):891-8. https://link.springer.com/article/10.1007/s10995-013-1315-9
Homer CJ, Klatka K, Romm D, Kuhlthau K, Bloom S, Newacheck P, Van Cleave J, Perrin JM. A review of the evidence for the medical home for children with special health care needs. Pediatrics. 2008 Oct;122(4):e922-37. http://pediatrics.aappublications.org/content/122/4/e922
MCHB-funded National Resource Center: National Center for Medical Home Implementation, https://medicalhomeinfo.aap.org/Pages/default.aspx
NPM-12 Transition
American Academy of Pediatrics, American Academy of Family Physicians, and American College of Physicians, Transitions Clinical Report Authoring Group. Clinical Report – Supporting the Health Care Transition from Adolescence to Adulthood in the Medical Home. Pediatrics. 2018: 142(5); e20182587; DOI: https://doi.org/10.1542/peds.2018-2587. https://pediatrics.aappublications.org/content/142/5/e20182587
American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics. 2002 Dec;110(6 Pt 2):1304-6. http://pediatrics.aappublications.org/content/110/Supplement_3/1304
Campbell F, Biggs K, Aldiss SK, O'Neill PM, Clowes M, McDonagh J, While A, Gibson F. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst Rev. 2016 Apr 29;4:CD009794. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009794.pub2/abstract
Gabriel P, McManus M, Rogers K, White P. Outcome Evidence for Structured Pediatric to Adult Health Care Transition Interventions: A Systematic Review. J Pediatr. 2017 Sep;188:263-269.e15. http://www.jpeds.com/article/S0022-3476(17)30759-X/fulltext
Schmidt A, Ilango SM, McManus MA, Rogers KK, White PH. Outcomes of Pediatric to Adult Health Care Transition Interventions: An Updated Systematic Review. J Pediatr Nurs. Mar-Apr 2020;51:92-107. doi: 10.1016/j.pedn.2020.01.002. Epub 2020 Jan 22. https://www.pediatricnursing.org/article/S0882-5963(19)30555-X/fulltext
NPM-13 Preventive Dental Visit
American Academy of Pediatric Dentistry. Guideline on Perinatal and Infant Oral Health Care. The Reference Manual of Pediatric Dentistry. 2016. https://www.aapd.org/globalassets/media/policies_guidelines/bp_perinataloralhealthcare.pdf
American College of Obstetricians and Gynecologists Women's Health Care Physicians; Committee on Health Care for Underserved Women. Committee Opinion No. 569: oral health care during pregnancy and through the lifespan. 2013, Reaffirmed 2017. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan
American Academy of Pediatric Dentistry. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. The Reference Manual of Pediatric Dentistry. 2018.
NPM-14 Smoking
The Health Consequences of Smoking—50 Years of Progress. A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. https://www.ncbi.nlm.nih.gov/books/NBK179276/pdf/Bookshelf_NBK179276.pdf
U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2006. https://www.ncbi.nlm.nih.gov/books/NBK44324/
NPM-15 Adequate Insurance
Kogan MD, Newacheck PW, Blumberg SJ, Ghandour RM, Singh GK, Strickland BB, van Dyck PC. Underinsurance among children in the United States. N Engl J Med. 2010 Aug 26;363(9):841-51. http://www.nejm.org/doi/full/10.1056/NEJMsa0909994
Smith PJ, Molinari NA, Rodewald LE. Underinsurance and pediatric immunization delivery in the United States. Pediatrics. 2009 Dec;124 Suppl 5:S507-14. http://pediatrics.aappublications.org/content/124/Supplement_5/S507.full
Smith PJ, Lindley MC, Shefer A, Rodewald LE. Underinsurance and adolescent immunization delivery in the United States. Pediatrics. 2009 Dec;124 Suppl 5:S515-21. http://pediatrics.aappublications.org/content/124/Supplement_5/S515.full
IOM (Institute of Medicine). 2009. America’s Uninsured Crisis: Consequences for Health and Health Care. Washington, DC: National Academies Press. https://pubmed.ncbi.nlm.nih.gov/25009923/
Table 4. National Performance and Outcome Measure Crosswalk to AMCHP Life Course Indicators
National Performance or Outcome Measure |
AMCHP Life Course Indicators |
||||
# |
Short Title |
Identifier |
Thematic Category |
Indicator Name |
Brief Description |
National Performance Measure |
|||||
4B |
Breastfeeding |
LC-27* |
Family Wellbeing |
Exclusive Breastfeeding at 3 Months |
Percent of children exclusively breastfed through 3 months |
6 |
Developmental screening |
LC-19** |
Early Life Services |
Early Childhood Health Screening - EPSDT |
Percent of Medicaid-enrolled children who received at least one initial or periodic screen in past calendar year |
8.2 |
Physical activity |
LC-33 * |
Family Wellbeing |
Physical Activity Among High School Students |
Proportion of high school students who are physically active for at least 60 minutes per day on five or more of the past seven days. |
9.1 |
Bullying |
LC-12 |
Discrimination and Segregation |
Bullying |
Percent of 9-12th graders who reported being bullied on school property or electronically bullied |
11 |
Medical home |
LC-37 |
Health Care Access and Quality |
Medical Home for Children |
Proportion of families who report their child received services in a medical home |
13.2 |
Preventive dental visit |
LC-41 |
Health Care Access and Quality |
Oral Health Preventive Visit for Children |
Percent of children who received a preventive dental visit in the past 12 months |
14.2 |
Smoking |
LC-28 |
Family Wellbeing |
Exposure to Second Hand Smoke in the Home |
Percent of children living in a household where smoking occurs inside home |
National Outcome Measure |
|||||
5 |
Preterm birth |
LC-55 |
Reproductive Life Experiences |
Preterm Birth |
Percent of live births born < 37 weeks gestation |
12 |
Newborn screening timely follow-up |
LC-17** |
Early Life Services |
Early Intervention |
Proportion of children aged 0-3 years who received EI services of all children aged 0-3 years |
16.3 |
Adolescent suicide |
LC-45* |
Mental Health |
Suicide |
Suicides per 100,000 population |
17.1 |
CSHCN |
LC-25 |
Family Wellbeing |
Children with Special Health Care Needs |
Percent of children (0-17 years) with a special health care need |
20.2 |
Obesity |
LC-32A |
Family Wellbeing |
Obesity |
Percent of children who are currently overweight or obese |
22.1 |
Child vaccination |
LC-35 |
Health Care Access and Quality |
Children Receiving Age Appropriate Immunizations |
Percent of children ages 19-35 receiving age-appropriate immunizations according to the Advisory Committee for Immunization Practices (ACIP) guidelines and HP 2020 Goal. |
Table 4. National Performance and Outcome Measure Crosswalk to AMCHP Life Course Indicators (Continued)
National Performance or Outcome Measure |
AMCHP Life Course Indicators |
||||
# |
Short Title |
Identifier |
Thematic Category |
Indicator Name |
Brief Description |
National Outcome Measure |
|||||
22.3 |
HPV vaccination |
LC-36A* |
Health Care Access and Quality |
Human Papillomavirus (HPV) Immunization |
The proportion of adolescents ages 13-17 who receive the evidence-based clinical preventive service HPV vaccine |
23 |
Teen births
|
LC-54* |
Reproductive Life Experiences |
Teen Births |
Number of live births born to women aged 10-19 years per 1,000 women aged 10-19 years |
24 |
Postpartum depression
|
LC-44 |
Mental Health |
Postpartum Depression |
Percent of women who have recently given birth who reported experiencing postpartum depression following a live birth |
25 |
Forgone health care |
LC-39* |
Health Care Access and Quality |
Inability or Delay in Obtaining Necessary Medical Care or Dental Care |
Percent of parents reporting their child was not able to obtain necessary medical care or dental care. |
*NPM or NOM similar to AMCHP indicator (different age range or definition)
**NPM or NOM conceptually related to AMCHP indicator
Source: http://www.amchp.org/programsandtopics/data-assessment/Pages/LifeCourseIndicators.aspx
APPENDIX C: |
DETAIL SHEETS FOR THE NATIONAL OUTCOME MEASURES AND NATIONAL PERFORMANCE MEASURES |
National Outcome Measures
National Performance Measures
A.
No. |
Title V MCH Services Block Grant - National Outcome Measures |
1 |
Percent of pregnant women who receive prenatal care beginning in the first trimester |
2 |
Rate of severe maternal morbidity per 10,000 delivery hospitalizations |
3 |
Maternal mortality rate per 100,000 live births |
4 |
Percent of low birth weight deliveries (<2,500 grams) |
5 |
Percent of preterm births (<37 weeks gestation) |
6 |
Percent of early term births (37,38 weeks gestation) |
7 |
Percent of non-medically indicated early elective deliveries |
8 |
Perinatal mortality rate per 1,000 live births plus fetal deaths |
9.1 |
Infant mortality rate per 1,000 live births |
9.2 |
Neonatal mortality rate per 1,000 live births |
9.3 |
Postneonatal mortality rate per 1,000 live births |
9.4 |
Preterm-related mortality rate per 100,000 live births |
9.5 |
Sudden Unexpected Infant Death (SUID) rate per 100,000 live births |
10 |
Percent of women who drink alcohol in the last 3 months of pregnancy |
11 |
Rate of neonatal abstinence syndrome per 1,000 birth hospitalizations |
12 |
Percent of eligible newborns screened for heritable disorders with on time physician notification for out of range screens who are followed up in a timely manner. (DEVELOPMENTAL) |
13 |
Percent of children meeting the criteria developed for school readiness (DEVELOPMENTAL) |
14 |
Percent of children, ages 1 through 17, who have decayed teeth or cavities in the past year |
15 |
Child mortality rate, ages 1 through 9, per 100,000 |
16.1 |
Adolescent mortality rate, ages 10 through 19, per 100,000 |
16.2 |
Adolescent motor vehicle mortality rate ages 15 through 19 per 100,000 |
16.3 |
Adolescent suicide rate ages 15 through 19 per 100,000 |
17.1 |
Percent of children with special health care needs (CSHCN), ages 0 through 17 |
17.2 |
Percent of children with special health care needs (CSHCN), ages 0 through 17, who receive care in a well-functioning system |
17.3 |
Percent of children, ages 3 through 17, diagnosed with an autism spectrum disorder |
17.4 |
Percent of children, ages 3 through 17, diagnosed with Attention Deficit Disorder/Attention Deficit Hyperactivity Disorder (ADD/ADHD) |
18 |
Percent of children, ages 3 through 17, with a mental/behavioral condition who receive treatment or counseling |
19 |
Percent of children, ages 0 through 17, in excellent or very good health |
20 |
Percent of children, ages 2 through 4, and adolescents, ages 10 through 17, who are obese (BMI at or above the 95th percentile) |
21 |
Percent of children, ages 0 through 17, without health insurance |
22.1 |
Percent of children who have completed the combined 7-vaccine series (4:3:1:3*:3:1:4) by age 24 months |
22.2 |
Percent of children, 6 months through 17 years, who are vaccinated annually against seasonal influenza |
22.3 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the HPV vaccine |
22.4 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the Tdap vaccine |
22.5 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the meningococcal conjugate vaccine |
23 |
Teen birth rate, ages 15 through 19, per 1,000 females |
24 |
Percent of women who experience postpartum depressive symptoms following a recent live birth |
25 |
Percent of children, ages 0 through 17, who were unable to obtain needed health care in the past year |
OUTCOME MEASURE 1 |
Percent of pregnant women who receive prenatal care beginning in the first trimester |

GOAL To ensure early entrance into prenatal care to enhance pregnancy outcomes. |
|
|
|
DEFINITION Numerator: Number of live births with reported first prenatal visit during the first trimester (before 13 weeks’ gestation)
Denominator: Number of live births
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) 08 Objective: Increase the proportion of pregnant women who receive early and adequate prenatal care. (Baseline: 76.4% of pregnant females received early and adequate prenatal care in 2018, Target: 80.5%) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Early prenatal care is essential for identification of maternal disease and risks for complications of pregnancy or birth. This can help ensure that women with complex problems, chronic illness, or other risks are seen by specialists. Early prenatal care can also provide important education and counseling on modifiable risks in pregnancy, including smoking, drinking, and inadequate or excessive weight gain.1 Although early high-quality prenatal care is essential, particularly for women with chronic conditions or other risk factors, it may not be sufficient to assure optimal pregnancy outcomes. Efforts to improve pregnancy outcomes and the health of mothers and infants should begin prior to conception, whether before a first or subsequent pregnancy2. As many women are not aware of being pregnant at first, it is important to establish healthy behaviors and achieve optimal health well before pregnancy.2 The timeliness of prenatal care measure for health plans is part of the Core Set of Maternal and Perinatal Health Measures for Medicaid and CHIP and the National Committee for Quality Assurance’s Healthcare Effectiveness Data and Information Set (HEDIS).
(1) National Institute of Child Health and Human Development. What is prenatal care and why is it important? 2017 January 31. https://www.nichd.nih.gov/health/topics/pregnancy/conditioninfo/prenatal-care
(2) Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care—United States. MMWR Recommendations and Reports. 2006;55(RR-06):1–23. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5506a1.htm |
|
OUTCOME MEASURE 2 |
Rate of severe maternal morbidity per 10,000 delivery hospitalizations |
GOAL To reduce life-threatening maternal illness and complications. |
|
|
|
DEFINITION Numerator: Number of delivery hospitalizations with an indication of severe morbidity from diagnosis or procedure codes (e.g. heart or kidney failure, stroke, embolism, hemorrhage).
Denominator: Number of delivery hospitalizations
Units: 10,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) 05 Objective: Reduce severe maternal complications identified during delivery hospitalizations. (Baseline: 68.7 per 10,000 delivery hospitalizations in 2017, Target: 61.8 per 10,000 delivery hospitalizations) |
|
|
|
DATA SOURCES Healthcare Cost and Utilization Project (HCUP) - State Inpatient Database (SID) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Over 25,000 women experience severe maternal morbidity during delivery hospitalizations every year. This includes significant life-threatening complications, such as hemorrhage, infection, and cardiac events, that may require lengthy hospital stays with long-term health consequences.1,2 Many more women require blood transfusions but there is significant under-reporting with the transition to ICD-10 coding and it may not reflect severe morbidity in the absence of other indicators. Rises in chronic conditions, including obesity, diabetes, hypertension, and cardiovascular disease, are likely to have contributed to rises in severe maternal morbidity.1 Minority women and particularly non-Hispanic black women have higher rates of severe maternal morbidity.2
|
|
OUTCOME MEASURE 3 |
Maternal mortality rate per 100,000 live births |
GOAL To reduce the maternal mortality rate. |
|
|
|
DEFINITION Numerator: Number of deaths related to or aggravated by pregnancy, but not due to accidental or incidental causes, and occurring within 42 days of the end of a pregnancy (follows WHO definition)
Denominator: Number of live births
Units: 100,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) 04 Objective: Reduce maternal deaths (Baseline: 17.4 maternal deaths per 100,000 live births in 2018, Target: 15.7 maternal deaths per 100,000 live births) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) for states and territories United Nations Maternal Mortality Estimation Interagency Group for the Freely Associated States in the Pacific Basin For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Maternal mortality is a sentinal indicator of health and health care quality worldwide. In 2018, the national maternal mortality rate was 17.4 deaths per 100,000 live births. There are significant racial disparities with Black women dying at more than 2.5 times the rate of White women (37.1 versus 14.7). Maternal deaths can be prevented or reduced both by improving underlying maternal health as well as health care quality for leading causes of maternal death, such as hemmorhage and preeclampsia.
|
|
|
|
OUTCOME MEASURE 4 |
Percent of low birth weight deliveries (<2,500 grams)
|
GOAL To reduce the percent of low birth weight deliveries |
|
|
|
DEFINITION Numerator: Number of live births weighing less than 2,500 grams
Denominator: Number of live births
Units: 100
Text: Percent
|
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) 07 Objective: Reduce preterm births. (Baseline: 10% of live births were preterm in 2018, Target: 9.4%) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Low birth weight infants include pre-term infants and infants with intrauterine growth retardation1. Some risk factors for low birth weight babies include: chronic health conditions, inadequate weight gain, both young and old maternal age, poverty, smoking, substance abuse, and multiple births.1 Low birth weight infants are more likely than normal weight infants to die in the first year of life and to experience long-range physical and developmental health problems.1 Infants born to non-Hispanic Black women have the highest rates of low birth weight, particularly very low birth weight, with levels that are about two or more times greater than for infants born to women of other race and ethnic groups.2
http://www.marchofdimes.org/baby/low-birthweight.aspx
|
|
OUTCOME MEASURE 5 |
Percent of preterm births (<37 weeks)
|
GOAL To reduce the percent of all preterm, early term, and early elective deliveries. |
|
|
|
DEFINITION Numerator: Number of live births before 37 completed weeks of gestation
Denominator: Number of live births
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) 07 Objective: Reduce preterm births. (Baseline: 10% of live births were preterm in 2018, Target: 9.4%) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Babies born preterm, before 37 completed weeks of gestation, are at greater risk of immediate life-threatening health problems, as well as long-term complications and developmental delays.1 Currently, about 1 in every 10 infants are born prematurely.1 Preterm birth is a leading cause of infant death and childhood disability, accounting for at least a third of all infant deaths.1 Infants born to non-Hispanic Black women have the highest rates of preterm birth, particularly early preterm birth, with levels that are at least 1.5 times those for infants born to women of other race and ethnic groups.2 Risk factors include infection, younger and older maternal age, substance use, poverty, stress, and multiple births.1
|
|
|
|
OUTCOME MEASURE 6 |
Percent of early term births (37,38 weeks) |
GOAL To reduce the percent of all preterm, early term, and early elective deliveries. |
|
|
|
DEFINITION Numerator: Number of live births born at 37,38 completed weeks of gestation
Denominator: Number of live births
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Although the risk is less than for preterm babies, those born “early term” at 37 or 38 completed weeks of gestation, are still at greater risk of immediate health problems and long-term complications compared to “full term” (39, 40 weeks completed gestation) infants.1 In 2018, more than 25% of all births were early term.2 Complications during the newborn period include respiratory distress and neurological disorder, while long-term complications can include learning and behavioral problems.1
|
|
|
|
OUTCOME MEASURE 7 |
Percent of non-medically indicated early elective deliveries |
GOAL To reduce the percent of all preterm, early term, and early elective deliveries. |
|
|
|
DEFINITION Numerator: Number of inductions or cesareans without labor or spontaneous rupture of membranes among deliveries at 37, 38 completed weeks of gestation without conditions possibly justifying elective delivery <39 weeks according to The Joint Commission
Denominator: Number of deliveries at 37, 38 completed weeks of gestation without conditions possibly justifying elective delivery <39 weeks according to The Joint Commission
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE |
|
|
|
DATA SOURCES CMS Hospital Compare For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Non-medically indicated early term births (37,38 weeks) present avoidable risks of neonatal morbidity and costly NICU admission.1 Early elective delivery prior to 39 weeks is a perinatal quality measure endorsed by the National Quality Forum (#469) and included within The Joint Commission’s National Quality Measures for hospitals (PC-01) and the Center for Medicare and Medicaid Services’ Hospital Inpatient Quality Reporting Program.2
|
|
|
|
OUTCOME MEASURE 8 |
Perinatal mortality rate per 1,000 live births plus fetal deaths |
GOAL To reduce the rate of perinatal deaths. |
|
|
|
DEFINITION Numerator: Number of fetal deaths 28 weeks or more gestation plus early neonatal deaths occurring under 7 days
Denominator: Number of live births plus fetal deaths at 28 weeks or more gestation
Units: 1,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) 01 Objective: Reduce the rate of fetal deaths at 20 or more weeks of gestation. (Baseline: 5.9 fetal deaths at 20 or more weeks of gestation per 1,000 live births and fetal deaths in 2017, Target: 5.7 fetal deaths at 20 or more weeks of gestation per 1,000 live births and fetal deaths)
Related to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births)
|
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Perinatal mortality is a reflection of the health of the pregnant woman and newborn as well as the quality of perinatal care. Risk factors for perinatal mortality include smoking during pregnancy, maternal obesity, uncontrolled hypertension or diabetes, infections and previous poor pregnancy outcome.1 Late fetal deaths are just as common as early neonatal deaths with a rate similar to overall infant mortality.1 The perinatal mortality rate is particularly high for non-Hispanic Black women, being more than twice the rate for non-Hispanic white women.2
|
|
OUTCOME MEASURE 9.1 |
Infant mortality rate per 1,000 live births |
GOAL To reduce the rate of infant death. |
|
|
|
DEFINITION Numerator: Number of deaths to infants from birth up to 1 year of age
Denominator: Number of live births
Units: 1,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) for states and territorities United Nations Interagency Group for Child Mortality Estimation for the Freely Associated States in the Pacific Basin For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Infant mortality, or the death of a child within the first year of life, is a sentinel measure of population health that reflects the underlying well-being of mothers and families, as well as the broader community and social environment that cultivate health and access to health-promoting resources.1 After a period of stagnation from 2000 to 2005, the U.S. infant mortality rate has continued to decline to record low levels below 6 per 1,000 live births.2 However, significant disparities continue to persist between racial groups, especially for infants born to non-Hispanic black, American Indian/Alaskan Native, Native Hawaiian/Other Pacific Islander, and Puerto Rican women.2 The infant mortality rate among non-Hispanic blacks is more than twice that of non-Hispanic whites.2 Leading causes of infant mortality include prematurity, birth defects, and sudden unexpected infant deaths. Infant mortality continues to be an extremely complex health issue with many medical, social, and economic determinants.
|
|
OUTCOME MEASURE 9.2 |
Neonatal mortality rate per 1,000 live births |
GOAL To reduce the rate of neonatal deaths. |
|
|
|
DEFINITION Numerator: Number of deaths to infants under 28 days
Denominator: Number of live births
Units: 1,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) for states and territorities United Nations Interagency Group for Child Mortality Estimation for the Freely Associated States in the Pacific Basin For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Neonatal deaths, within the first month of life, account for approximately two-thirds of all infant deaths in the U.S.1 Neonatal mortality is related to gestational age, low birth weight, congenital malformations and health problems originating in the perinatal period, such as infections or birth trauma.2 A significant disparity exists in neonatal deaths between racial groups, especially for infants born to Black women. Infants born to non-Hispanic black women have the highest neonatal mortality rate, more than twice that for non-Hispanic white women.1 Neonatal mortality rates are also higher for infants born to Puerto Rican, American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander and Mexican women compared to non-Hispanic white women.1
|
|
|
|
OUTCOME MEASURE 9.3 |
Postneonatal mortality rate per 1,000 live births |
GOAL To reduce the rate of postneonatal deaths.
|
|
DEFINITION Numerator: Number of deaths to infants from 28 days up to 1 year of age
Denominator: Number of live births
Units: 1,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Postneonatal deaths, which occur from one month up to one year after birth, account for approximately one-third of all infant deaths in the U.S.1 Postneonatal mortality is generally related to Sudden Unexpected Infant Death (SUID)/Sudden Infant Death Syndrome (SIDS), unintentional injuries and congenital malformations.2 Similar to overall infant mortality, infants of non-Hispanic black and American Indian/Alaska Native women have the highest postneonatal mortality rates of any group—more than twice those for non-Hispanic white women.1
|
|
|
|
OUTCOME MEASURE 9.4 |
Preterm-related mortality rate per 100,000 live births |
GOAL To reduce the rate of preterm-related death. |
|
|
|
DEFINITION Numerator: Number of deaths due to preterm-related causes, following the CDC definition of underlying causes where 75% or more of total infant deaths attributed to that cause were deaths of infants born preterm (<37 weeks of gestation) and the cause of death was a direct consequence of preterm birth based on a clinical evaluation and review of the literature
Denominator: Number of live births
Units: 100,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births)
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Preterm birth is a leading cause of infant mortality, accounting for approximately one-third of all infant deaths.1 Preterm-related mortality can be prevented both by reducing preterm birth as well as improving access to risk-appropriate perinatal care for infants born prematurely.2 Similar to preterm birth and overall infant mortality, there are significant racial/ethnic disparities in preterm-related mortality. Preterm-related mortality rates are highest for infants born to non-Hispanic black and Puerto Rican women, with rates that are approximately 3 and 2 times higher than non-Hispanic white women.1 Preterm-related deaths account for the majority of the overall infant mortality gap for both non-Hispanic black and Puerto Ricans compared with non-Hispanic whites.1
|
|
|
|
OUTCOME MEASURE 9.5 |
Sudden Unexpected Infant Death (SUID) rate per 100,000 live births |
GOAL To reduce the rate sleep-related infant deaths |
|
|
|
DEFINITION Numerator: Number of SUID deaths, including SIDS (R95), unknown cause (R99), and accidental suffocation and strangulation in bed (W75)
Denominator: Number of live births
Units: 100,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 02: Reduce the rate of infant deaths within 1 year of age. (Baseline: 5.8 infant deaths per 1,000 live births within the first year of life in 2017, Target: 5.0 infant deaths per 1,000 live births) |
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Sleep-related infant deaths, also called Sudden Unexpected Infant Deaths (SUID) account for the largest share of infant deaths from one month up to one year (postneonatal deaths).1 Similar to overall infant mortality, SUID rates vary greatly by race and ethnicity, with infants born to American Indian/Alaska Native and non-Hispanic Black mothers having more than twice the rate among infants born to non-Hispanic whites.1,2 To reduce SUIDs, the American Academy of Pediatrics recommends safe sleep practices, such as placing babies to sleep on their backs on a separate firm sleep surface without soft objects or loose bedding, as well as other protective practices such as breastfeeding and smoking cessation.1
|
|
|
|
OUTCOME MEASURE 10 |
Percent of women who drink alcohol in the last 3 months of pregnancy
|
GOAL To reduce the percent of infants born with fetal alcohol spectrum disorders
|
|||
DEFINITION Numerator: Number of women who report drinking alcohol in the last 3 months of pregnancy
Denominator: Number of women with a recent live birth
Units: 100
Text: Percent |
|||
|
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) 09: Increase abstinence from alcohol among pregnant women. (Baseline: 89.3% of pregnant females aged 15 to 44 years reported abstaining from alcohol in the past 30 days in 2017-18, Target: 92.2%) |
|||
|
|
||
DATA SOURCES Pregnancy Risk Assessment Monitoring System (PRAMS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|||
|
|
||
SIGNIFICANCE Fetal alcohol spectrum disorders (FASDs), which result in life-long physical and cognitive and/or behavioral problems, are caused by drinking during pregnancy.1 In 2015-2017, around 1 in 9 pregnant women reported drinking alcohol in the past 30 days, and a third of those women reported binge drinking.2 Fetal alcohol syndrome (FAS) represents the severe end of FASDs, and is characterized by abnormal facial features (e.g., smooth ridge between nose and upper lip), lower than average height or weight, and central nervous system problems that create deficits in learning, memory, attention, communication, vision, and/or hearing.1 FASDs are preventable through abstinence from alcohol among pregnant women. Early diagnosis and intervention programs are critical to improve developmental outcomes for children with FAS.1
|
|||
|
|
||
OUTCOME MEASURE 11 |
Rate of neonatal abstinence syndrome per 1,000 birth hospitalizations
|
GOAL To reduce the rate of infants born with drug dependency.
|
|
DEFINITION Numerator: Number of birth hospitalizations with a diagnosis code of neonatal abstinence syndrome
Denominator: Number of birth hospitalizations
Units: 1,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health Objective 11: Increase abstinence from illicit drugs among pregnant women. (Baseline: 93.0% in 2017-18; Target: 95.3%) |
|
|
|
DATA SOURCES Healthcare Cost and Utilization Project (HCUP) - State Inpatient Database (SID) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures
SIGNIFICANCE Neonatal drug dependency or withdrawal symptoms, known as neonatal abstinence syndrome (NAS), predominantly occur from maternal use of opiates such as heroin, methadone, and prescription pain medications. Symptoms of NAS include fever, gastrointestinal dysfunction, high-pitched continuous crying, tremors, and feeding difficulties.1 From 2004 to 2014, the incidence of NAS increased more than five-fold, driven in large part by increases among Medicaid-financed births.2 Prevention strategies exist along the continuum from preconception, prenatal, postpartum, and infant/childhood stages to help avert substance-exposed pregnancies and improve outcomes for infants born with NAS.1
|
|
OUTCOME MEASURE 12 |
Percent of eligible newborns screened for heritable disorders with on time physician notification for out of range screens who are followed up in a timely manner. (DEVELOPMENTAL) |
GOAL To increase the percent of eligible newborns screened for heritable disorders with on-time physician notification for out of range screens and timely follow up. |
|
|
|
DEFINITION Numerator: Number of eligible newborns screened for heritable disorders with on time physician notification for out of range screens who are followed up in a timely manner. UNDER DEVELOPMENT.
Denominator: Number of live eligible births
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE |
|
|
|
DATA SOURCES The American Public Health Laboratories (APHL) data set |
|
|
|
SIGNIFICANCE Newborn screening detects thousands of babies each year with potentially devastating, but treatable disorders. The benefits of newborn screening depend upon timely collection of the newborn blood-spots or administration of a point-of-care test (pulse oximeter for critical congenital heart disease (CCHD)), receipt of the newborn blood spot at the laboratory, testing of the newborn blood spot, and reporting out of all results. Timely detection and follow-up with appropriate treatment prevents death or disability and enables children to reach their full potential.
|
|
|
|
OUTCOME MEASURE 13 |
Percent of children meeting the criteria developed for school readiness (DEVELOPMENTAL) |
GOAL To increase the percent of children ready for school. |
|
|
|
DEFINITION Numerator: Under development
Denominator: Under development
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE |
|
Related to Early and Middle Childhood (EMC) Objective D01: Increase the proportion of children who are developmentally on track and ready for school. (Developmental)
|
|
DATA SOURCES National Survey of Children's Health (NSCH)
|
|
For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures
|
|
SIGNIFICANCE Early childhood is a critical period where experiences impact the structural development of the brain and neurobiological pathways for functional development. Studies have shown that children’s early learning skills, self-regulation, social emotional development and motor skills at school entry are good predictors of later academic achievement, high levels of education and secure employment. Social gradients in language and literacy, communication and socioemotional functioning emerge early for children across socioeconomic backgrounds, and these differences persist into the school years. Interventions such as home visiting or high-quality preschool may help reduce these disparities, and act as a protective factor against the future onset of adult disease and disability. However, disparities persist in children’s access to supportive, nurturing environments and experiences that can optimize development and mitigate risk factors. Efforts to expand and ensure equitable receipt of high-quality early childhood programs may increase development of school readiness skills among young children, setting the stage for optimal learning later in life.
|
|
|
|
OUTCOME MEASURE 14 |
Percent of children, ages 1 through 17, who have decayed teeth or cavities in the past year |
GOAL To reduce the percent of children and adolescents who have dental caries or decayed teeth. |
|
|
|
DEFINITION Numerator: Number of children, ages 1 through 17, who are reported by a parent to have frequent or chronic difficulty with decayed teeth or cavities in the past year
Denominator: Number of children, ages 1 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Oral Health of Children and Adolescents (OH) Objective 01: Reduce the proportion of children and adolescents with lifetime tooth decay experience in their primary or permanent teeth. (Baseline: 48.4% in 2013-16, Target: 42.9%)
Related to Oral Health of Children and Adolescents (OH) Objective 02: Reduce the proportion of children and adolescents with active and currently untreated tooth decay in their primary or permanent teeth. (Baseline 13.4% in 2013-16, Target: 10.2%)
|
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Tooth decay (cavities) is among the most common chronic conditions of childhood. Untreated tooth decay can lead to pain and infections which may result in problems with eating, speaking, learning and playing. Children with poor oral health tend to miss more school and get lower grades than those who do not. Tooth decay can be prevented through recommended preventive dental care, including flouride varnish and dental sealants, community water flouridation, and oral hygeine practices, including brushing and flossing.
|
|
|
|
OUTCOME MEASURE 15 |
Child mortality rate, ages 1 through 9, per 100,000 |
GOAL To reduce the death rate of children, ages 1 through 9. |
|||
|
|
||
DEFINITION Numerator: Number of deaths among children, ages 1 through 9 years
Denominator: Number of children, ages 1 through 9 years
Units: 100,000
Text: Rate |
|||
|
|
||
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 03: Reduce the rate of deaths among children and adolescents aged 1 to 19 years. (Baseline: 25.2 deaths among children and adolescents aged 1 to 19 years per 100,000 population occurred in 2018, Target: 18.4 deaths per 100,000 population) |
|||
|
|
||
DATA SOURCES National Vital Statistics System (NVSS) Population estimates come from the U.S. Census Bureau For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|||
|
|
||
SIGNIFICANCE Although the risk of death for children declines sharply beyond infancy, there were still over 6,000 deaths among U.S. children ages 1 through 9 in 2017. Unintentional injury continues to be the leading cause of death in children 1 to 9 years. Other leading causes include congenital malformations, malignant neoplasms, and homicide.
|
|||
|
|
||
|
|
|
|
OUTCOME MEASURE 16.1 |
Adolescent mortality rate, ages 10 through 19, per 100,000
|
GOAL To reduce the death rate of adolescents, ages 10 through 19. |
|
|
|
DEFINITION Numerator: Number of deaths among adolescents, ages 10 through 19 years
Denominator: Number of adolescents, ages 10 through 19 years
Units: 100,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 03: Reduce the rate of deaths among children and adolescents aged 1 to 19 years. (Baseline: 25.2 deaths among children and adolescents aged 1 to 19 years per 100,000 population occurred in 2018, Target: 18.4 deaths per 100,000 population)
|
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) Population estimates come from the U.S. Census Bureau For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Although the risk of death declines sharply in early childhood, mortality rates begin to increase again in adolescence. Over 14,000 deaths occurred among U.S. children ages 10 through 19 in 2017. The leading causes of illness and death among adolescents and young adults are largely preventable. Unintentional injury continues to be the leading cause of death in adolescents 10 to 19 years, followed by suicide, homicide, and malignant neoplasms.
|
|
|
|
OUTCOME MEASURE 16.2 |
Adolescent motor vehicle mortality rate, ages 15 through 19, per 100,000
|
GOAL To reduce the death rate of adolescents, ages 15 through 19, from motor vehicle crashes |
|
|
|
DEFINITION Numerator: Number of deaths to adolescents, ages 15 through 19 years, caused by motor vehicle crashes. This includes all occupant, pedestrian, motorcycle, bicycle, etc. deaths caused by motor vehicles.
Denominator: Number of adolescents, ages 15 through 19 years
Units: 100,000
Text: Rate |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Objective Injury and Violence Prevention (IVP) 06: Reduce motor vehicle crash-related deaths. (Baseline: 11.2 motor vehicle traffic-related deaths per 100,000 population occurred in 2018 (age adjusted to the year 2000 standard population), Target: 10.1 per 100,000 population)
|
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) Population estimates come from the U.S. Census Bureau For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE More than one-third of all teen deaths are the result of a motor vehicle crash. Teenage drivers have crash rates that are nearly three times those of drivers older than 20 years.1 Factors related to lack of driving experience and maturity contribute to motor vehicle mortality, such as speeding, distracted driving, reckless driving, impaired driving, not wearing seatbelts, and presence of other teenage passengers.1 Males ages 16-19 are more than twice as likely to die in motor vehicle accidents as females the same age.1
|
|
|
|
OUTCOME MEASURE 16.3 |
Adolescent suicide rate, ages 15 through 19, per 100,000 |
GOAL To eliminate self-induced, preventable morbidity and mortality. |
||
|
|
|
DEFINITION Numerator: Number of deaths attributed to suicide among adolescents ages 15 through 19 years
Denominator: Number of adolescents, ages 15 through 19 years
Units: 100,000
Text: Rate |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Mental Health and Mental Disorders (MHMD) Objective 01: Reduce the suicide rate. (Baseline: 14.2 suicides per 100,000 population occurred in 2018 (age adjusted to the year 2000 standard population), Target: 12.8 suicides per 100,000 population)
Related to MHMD Objective 02: Reduce suicide attempts by adolescents. (Baseline: 2.4 suicide attempts per 100 population of students in grades 9 through 12 occurred in the past 12 months, as reported in 2017, Target: 1.8 suicide attempts per 100) |
||
DATA SOURCES National Vital Statistics System (NVSS) Population estimates come from the U.S. Census Bureau For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
||
|
|
|
SIGNIFICANCE Suicide is the second leading cause of death for adolescents ages 15 through 19 years.1 In 2017, there were 3,948 deaths due to suicide among adolescents ages 15 to 19 years, or 11.8 deaths per 100,000.1 Adolescent suicide increased 56% between 2007 and 2017.2 Suicide and suicidal ideation is often indicative of mental health problems and stressful or traumatic life events. In 2017,17.2 percent of high school students reported they had thought seriously about committing suicide in the past year.3 While females are more likely to report considering suicide,3 males are more likely to succeed in committing suicide.1 The suicide mortality rate for males is nearly three times that of females.1
|
||
OUTCOME MEASURE 17.1 |
Percent of children with special health care needs (CSHCN), ages 0 through 17 |
|
GOAL To track the percent of children and youth with special health care needs). |
|
|
|
DEFINITION Numerator: Number of children, ages 0 through 17, who are reported by a parent to meet the criteria for having a special health care need based on the CSHCN screener (need for or use of prescription medication, elevated need for or use of services, functional limitations, need for or use of specialized therapy, ongoing emotional, behavioral, or developmental problems for which treatment or counseling is needed)
Denominator: Number of children, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE |
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Children are considered to have a special health care need if, in addition to a chronic medical, behavioral, or developmental condition that has lasted or is expected to last 12 months or longer, they experience either service-related or functional consequences, including the need for or use of prescription medications and/or specialized therapies.1 About 1 in 5 of all US children are considered to have special health care needs. However, they account for almost half of all health care expenditures for children.2
|
|
|
|
OUTCOME MEASURE 17.2 |
Percent of children with special health care needs (CSHCN), ages 0 through 17, who receive care in a well-functioning system |
GOAL To ensure access to needed and continuous systems of care for children and youth with special health care needs. |
|
|
|
DEFINITION Numerator: Number of CSHCN, ages 0 through 17, who are reported by a parent to receive all components of a well-functioning system of care (families partner in decision-making if needed, medical home, preventive medical and dental care, continuous and adequate insurance, easy access to services, and preparation for transition to adult health care among adolescents)
Denominator: Number of CSHCN, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) Objective 20: Increase the proportion of children and adolescents with special health care needs who receive care in a family-centered, comprehensive, and coordinated system. (Baseline: 15.7% in 2016-17, Target: 19.5%) |
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE According to the 2017-18 NSCH, only 13.9% of CSHCN receive services in a well-functioning system of services. The Omnibus Budget Reconciliation Act of 1989 requires Title V to provide and promote family-centered, community-based, coordinated care and facilitate the development of community-based systems of services for children with special health care needs and their families. To address this requirement a minimum of 30 percent of the Title V Block Grant funding is allocated for this purpose, and HP 2030 Objective MICH-19 establishes the goal to increase the proportion of children with special health care needs who receive their care in family-centered, comprehensive, and coordinated systems.
|
|
OUTCOME MEASURE 17.3 |
Percent of children, ages 3 through 17, diagnosed with an autism spectrum disorder |
GOAL To track the percent of children and youth with autism spectrum disorder (ASD). |
|
|
|
DEFINITION Numerator: Number of children, ages 3 through 17, who are reported by a parent to have ever been told they have autism or ASD by a health care provider and to currently have the condition
Denominator: Number of children, ages 3 through17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Autism spectrum disorder (ASD) is a developmental disability that can cause significant social, communication and behavioral challenges. The prevalence of ASD has risen sharply over the last two decades. Aproximately 1 in 54 8-year old children have ASD. ASD is 4 times more common among boys than girls. While ASD can be detected by 18 months or earlier, the average age at diagnosis for ASD is 4 years old.The American Academy of Pediatrics recommends screening for ASD at 18 and 24 months. Early intervention services can improve a child’s development.
|
|
OUTCOME MEASURE 17.4 |
Percent of children, ages 3 through 17, diagnosed with Attention Deficit Disorder/Attention Deficit Hyperactivity Disorder (ADD/ADHD) |
GOAL To track the percent of children and youth with attention deficit disorder/attent deficit hyperactivity disorder (ADD/ADHD). |
|
|
|
DEFINITION Numerator: Number of children, ages 3 through 17, who are reported by a parent to have ever been told they have ADD or ADHD by a health care provider and to currently have the condition
Denominator: Number of children, ages 3 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurobehavioral disorders of childhood. It is sometimes referred to as Attention Deficit Disorder (ADD). ADHD is usually first diagnosed in childhood and often lasts into adulthood. Children with ADHD may have trouble paying attention, controlling impulsive behaviors, or be overly active. Children with ADHD are at increased risk for mental, behavioral, and emotional concerns and disorders. In 2017-2018, over 5 million children 3-17 years (8.9%) were currently diagnosed with ADHD.
|
|
|
|
OUTCOME MEASURE 18 |
Percent of children, ages 3 through 17, with a mental/behavioral condition who receive treatment or counseling |
GOAL To increase the percent of children with a mental/behavioral condition who receive treatment or counseling. |
|
|
|
DEFINITION Numerator: Number of children, ages 3 through 17, who are reported by a parent to have ever been told they have a mental/behavioral condition by a health care provider (depression, anxiety problems, or behavioral or conduct problems), to currently have the condition, and to have received treatment or counseling from a mental health professional in the past year
Denominator: Number of children, ages 3 through 17, who are reported by a parent to have ever been told they have a mental/behavioral condition by a health care provider (depression, anxiety problems, or behavioral or conduct problems) and to currently have the condition
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Mental Health and Mental Disorders (MHMD) Objective 03: Increase the proportion of children with mental health problems who get treatment. (Baseline: 73.3% of children aged 4 to 17 years with mental health problems received treatment in 2018, Target: 82.4%) |
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Mental disorders among children are described as serious changes in the way children typically learn, behave, or handle their emotions, which cause distress and problems getting through the day.1 The prevalence of mental/behavioral health conditions has been increasing among children and has been found to vary by geographic and sociodemographic factors.2 However, a significant portion of children diagnosed with a mental health condition do not receive treatment.2 Further, the receipt of treatment is generally dependent on sociodemographic and health-related factors.2 Adequate insurance and access to a patient-centered medical home may improve mental health treatment.
|
|
|
|
OUTCOME MEASURE 19 |
Percent of children, ages 0 through 17, in excellent or very good health |
GOAL To improve the health status of children. |
|
|
|
DEFINITION Numerator: Number of children, ages 0 through 17, who are reported by a parent to be in excellent or very good health
Denominator: Number of children, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Overall health status for children provides a global, summary measure of children’s health and well-being. Children reported to be in excellent or very good health are more likely to thrive in a variety of health dimensions, including physical and mental health. Self or proxy-reported health status is an indicator of health-related quality of life that is often more predictive of morbidity and mortality than objective measures of health.
|
|
|
|
OUTCOME MEASURE 20 |
Percent of children, ages 2 through 4, and adolescents, ages 10 through 17, who are obese (BMI at or above the 95th percentile) |
|
GOAL To reduce the percent of children and adolescents who are considered obese. |
||
|
|
|
DEFINITION Numerators: Number of children, ages 2 through 4, who are obese based on measured height and weight (WIC) Number of adolescents, ages 10 through 17, who are obese based on parent-reported height and weight (NSCH) Number of adolescents in grades 9 through 12 who are obese based on self-reported height and weight (YRBSS)
Denominators: Number of children, ages 2 through 4 (WIC) Number of adolescents, ages 10 through 17 (NSCH) Number of adolescents in grades 9 through 12 (YRBSS) Units: 100
Text: Percent |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Nutrition and Weight Status (NWS) Objective 04: Reduce the proportion of children and adolescents with obesity. (Baseline: 17.8% of children and adolescents aged 2 to 19 years had obesity in 2013-16, Target: 15.5%) |
||
|
|
|
DATA SOURCES Children 2-4 years: Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Adolescents 10 through 17 years (parent report): National Survey of Children’s Health (NSCH) Adolescents grades 9 through 12 (adolescent report): Youth Risk Behavior Surveillance System (YRBSS)
For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures
|
||
|
|
|
SIGNIFICANCE Childhood obesity is defined as a body mass index (BMI) at or above the 95th percentile for children and teens of the same age and sex.1 Childhood obesity is a serious health problem in the United States, that has tripled in prevalence since the 1970s.1 Currently, about 1 in 5 school-aged children are obese.1 Childhood obesity is associated with a variety of adverse consequences, including an increased risk of cardiovascular disease, type 2 diabetes, asthma, social stigmatization, low self-esteem, and adult obesity.1 Obesity in adulthood is linked to cardiovascular disease, type 2 diabetes, and cancer, and obese children are likely to have more severe obesity and attendant health problems in adulthood.1
|
||
OUTCOME MEASURE 21 |
Percent of children, ages 0 through 17, without health insurance |
GOAL To ensure access to needed health care services for children.
|
|
DEFINITION Numerator: Number of children, ages 0 through 17, who are reported by a parent to not be currently covered by any private or public health insurance
Denominator: Number of children, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Access to Health Services (AHS) Objective 01: Increase the proportion of persons with medical insurance. (Baseline: 89.0% of persons under 65 years had medical insurance in 2018, Target: 92.1%) |
|
|
|
DATA SOURCES American Community Survey (ACS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE There is a well documented benefit for children in having health insurance. Research has shown that children who acquire health insurance are more likely to have access to a usual source of care, receive well child care and immunizations, to have developmental milestones monitored, and receive prescriptions drugs, appropriate care for asthma and basic dental services.1 Serious childhood problems are more likely to be identified early in children with insurance, and insured children with special health care needs are more likely to have access to specialists.1 Insured children not only receive more timely diagnosis of serious health care conditions but experience fewer avoidable hospitalizations, improved asthma outcomes and fewer missed school days.1 The number of uninsured children in the United States decreased for many years, reaching the lowest percent in 2016 at 4.7%.2 However, between 2016 and 2018 the number of uninsured children increased by 12.5%, largely due to a decline in public coverage.2
|
|
|
|
|
Percent of children who have completed the combined 7-vaccine series (4:3:1:3*:3:1:4) by age 24 months
|
GOAL To increase the percent of children and adolescents who have completed recommended vaccines. |
|
|
|
DEFINITION Numerator: Number of children who have completed the combined 7-vaccine series of routinely recommended vaccinations (4:3:1:3*:3:1:4) by age 24 months
Denominator: Number of children born in a calendar year
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Immunization and Infectious Disease (IID) Objective 06: Increase the vaccination coverage level of 4 doses of the diphtheria-tetanus-acellular pertussis (DTaP) vaccine among children by age 2 years. (Baseline: 80.7% of children born in 2015 received 4 or more doses of DTaP by their 2nd birthday, Target: 90.0%)
Related to IID Objective 03: Maintain the vaccination coverage level of 1 doses of the measles-mumps-rubella (MMR) vaccine among children by age 2 years. (Baseline: 90.8% of children born in 2015 received at least 1 does of MMR by their 2nd birthday, Target: 90.8%)
Related to IID Objective 02: Reduce the proportion of children who receive 0 doses of recommended vaccines by age 2 years. (Baseline: 1.3% of children born in 2015 had received 0 doses of recommended vaccines by their 2nd birthday, Target: 1.3%) |
|
|
|
DATA SOURCES National Immunization Survey (NIS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Vaccination is one of the greatest public health achievements of the 20th century, resulting in dramatic declines in morbidity and mortality for many infectious diseases.1 Childhood vaccination in particular is considered among the most cost-effective preventive services available, as it averts a potential lifetime lost to death and disability.2 Currently, there are 15 different vaccines recommended by the Centers for Disease Control and Prevention from birth through age 18, many of which require multiple doses for effectiveness as well as boosters to sustain immunity.3
|
|
|
|
OUTCOME MEASURE 22.2 |
Percent of children, ages 6 months through 17 years, who are vaccinated annually against seasonal influenza
|
|
GOAL To increase the percent of children and adolescents who have completed recommended vaccines. |
||
|
|
|
DEFINITION Numerator: Number of children, ages 6 months through 17 years, who are reported by a parent to have received a seasonal influenza vaccine
Units: 100
Text: Percent |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Immunization and Infectious Disease (IID) Objective 09: Increase the proportion of persons who are vaccinated annually against seasonal influenza. (Baseline of 49.2% of persons aged 6 months and over were vaccinated against seasonal influenza for the flu season 2017-18, Target: 70.0%) |
||
|
|
|
DATA SOURCES National Immunization Survey - Flu (NIS-Flu) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
||
|
|
|
SIGNIFICANCE
Influenza (flu) is a contagious respiratory illness caused by influenza viruses.1 Influenza can cause mild to severe illness.1 Each year, millions of children get sick with seasonal flu; thousands of children are hospitalized, and some children die from the flu.2 Possible complications from the flu include: pneumonia, dehydration, worsening long-term medical problems, brain dysfunction, sinus problems and ear infections, and death.2 Annual flu vaccinaion helps prevent flu infection and risk of flu-associated hospitalization.1
|
||
|
|
|
OUTCOME MEASURE 22.3 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the HPV vaccine |
GOAL To increase the percent of children and adolescents who have completed recommended vaccines. |
|
|
|
DEFINITION Numerator: Number of adolescents, ages 13 through 17, who have received at least one dose of the HPV vaccine
Denominator: Number of adolescents, ages 13 through 17 years
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Immunization and Infectious Disease (IID) Objective 08: Increase the proportion of adolescents who receive recommended doses of human papillomavirus (HPV) vaccine. (Baseline 48.0% of adolescents aged 13 through 15 years received recommended doses of the HPV vaccine in 2018, Target: 80.0%) |
|
|
|
DATA SOURCES National Immunization Survey - Teen (NIS-Teen) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE
HPV (Human papillomavirus) vaccine can prevent infection with some types of human papillomavirus that are spread through intimate skin-to-skin or sexual contact.1 HPV vaccine prevents infection from HPV types that cause over 90% of the following cancers: cervical, vaginal and vuvlvar cancers in women; penile cancer in men; and anal cancers in both men and women.1 HPV is recommended for adolescents 11 or 12 years of age to ensure protection before exposure to the virus.1
|
|
|
|
OUTCOME MEASURE 22.4 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the Tdap vaccine
|
GOAL To increase the percent of children and adolescents who have completed recommended vaccines. |
|
|
|
DEFINITION Numerator: Number of adolescents, ages 13 through 17, who have received at least one dose of the Tdap vaccine
Denominator: Number of adolescents, ages 13 through 17 years
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
|
|
|
DATA SOURCES National Immunization Survey - Teen (NIS-Teen) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE
Tdap vaccine protects against tetanus, diphtheria, and pertussis.1 Vaccination has helped keep the incidence of these diseases low in the United States. Infants and young children are recommended to receive a 5-dose series of diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccines, with one adolescent booster dose of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine.2
|
|
|
|
OUTCOME MEASURE 22.5 |
Percent of adolescents, ages 13 through 17, who have received at least one dose of the meningococcal conjugate vaccine
|
|
GOAL To increase the percent of children and adolescents who have completed recommended vaccines. |
||
|
|
|
DEFINITION Numerator: Number of adolescents, ages 13 through17, who have received at least one dose of the meningococcal conjugate vaccine
Denominator: Number of adolescents, ages 13 through 17 years
Units: 100
Text: Percent |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
||
|
|
|
DATA SOURCES National Immunization Survey - Teen (NIS-Teen) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
||
|
|
|
SIGNIFICANCE
Meningococcal disease can cause meningitis (infection of the lining of the brain and spinal cord) and infections of the blood.1,2 Even when it is treated, meningococcal disease kills 10 to 15 infected people out of 100. 1,2 And of those who survive, about 10 to 20 out of every 100 will suffer disabilities such as hearing loss, brain damage, kidney damage, loss of limbs, nervous system problems, or severe scars from skin grafts. 1,2
|
||
OUTCOME MEASURE 23 |
Teen birth rate, ages 15 through 19, per 1,000 females
|
|
GOAL To reduce pregnancies to teenagers. |
||
|
|
|
DEFINITION Numerator: Number of births to adolescents, ages 15 through 19 years
Denominator: Number of adolescent females, ages 15 through 19 years
Units: 1,000
Text: Rate |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Family Planning (FP) 03: Reduce pregnancies among adolescent females. (Baseline: 43.4 pregnancies per 1,000 females aged 15 to 19 years occurred in 2013, Target 31.4 pregnancies per 1,000 females) |
||
|
|
|
DATA SOURCES National Vital Statistics System (NVSS) for states and territories Population estimates come from the U.S. Census Bureau United Nations Population Division for the Freely Associated States in the Pacific Basin
For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
||
|
|
|
SIGNIFICANCE Teen pregnancy and childbearing have substantial social and economic costs for both teens and their children. Teen mothers are less likely to complete high school and further education which may reduce earning potential and contribute to intergenerational poverty. Although teen pregnancy and birth rates have declined substantially over the past two decades, rates are still higher than in many other industrialized countries and large racial/ethnic disparities persist. Birth rates for American Indian/Alaska Native, non-Hispanic Black, Native Hawaiian/Other Pacific Islander, and Hispanic teens are approximately double that of non-Hispanic White teens.
|
||
OUTCOME MEASURE 24 |
Percent of women who experience postpartum depressive symptoms following a recent live birth
|
GOAL To reduce the prevalence of postpartum depression |
|
|
|
DEFINITION Numerator: Number of women who report postpartum depressive symptoms following a recent live birth (defined as reporting always/often feeling down, depressed, hopeless or always/often having little interest or little pleasure in doing things)
Denominator: Number of women with a recent live birth
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
|
|
|
DATA SOURCES Pregnancy Risk Assessment Monitoring System (PRAMS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Postpartum depression (PPD) is common, affecting as many as 1 in 7 mothers.1 PPD generally occurs within 4 to 6 weeks after childbirth with symptoms that may include depressed mood, loss of interest or pleasure in activities, sleep disturbance, appetite disturbance, loss of energy, feelings of worthlessness or guilt, diminished concentration, irritability, anxiety, and thoughts of suicide.1 PPD is associated with negative maternal physical and psychological health, relationship problems, and risky behaviors.2 PPD is associated with poor maternal and infant bonding and may negatively influence child development.2 Infant consequences of PPD include less infant weight gain and stunting, problems with sleep, poor social, emotional, behavioral, cognitive, and language development.2 Universal screening and treatment for pregnant and postpartum women is recommended by the American College of Obstetricians and Gynecologists (ACOG), the American Academy of Pediatrics (AAP), and the U.S. Preventive Services Task Force.1
|
|
OUTCOME MEASURE 25 |
Percent of children, ages 0 through 17, who were unable to obtain needed health care in the past year
|
GOAL To ensure access to needed health care services for children. |
|
|
|
DEFINITION Numerator: Number of children, ages 0 through 17 years, who are reported by a parent to be unable to obtain needed health care in the past year
Denominator: Number of children, ages 0 through 17 years
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Access to Health Services (AHS) Objective 04: Reduce the proportion of persons who are unable to obtain or delay in obtaining necessary medical care. (Baseline 4.1% of persons unable to obtain or delayed in obtaining necessary medical care in 2017, Target 3.3%)
Related to AHS 05: Reduce the proportion of persons who are unable to obtain or delayed in obtaining necessary dental care. (Baseline 4.6% in 2017, Target 4.1%)
Related to AHS 06: Reduce the proportion of persons who are unable to obtain or delayed in obtaining necessary prescription medicines. (Baseline 3.4 % in 2017, Target 3.0%) |
|
|
|
DATA SOURCES National Survey of Children’s Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
|
|
SIGNIFICANCE Improving access to quality health services is essential for optimal health in both preventing and treating health conditions. When needed care is not received, health may suffer and conditions may not be prevented or may grow in severity. Common barriers to care include financial burden, insurance coverage, insurance type, language, and parental education.2,3 Adequate insurance and access to a patient-centered medical home can reduce unmet needs for health care.1
|
|
B.
Title V MCH Services Block Grant National Performance Measures |
|
No. |
National Performance Measure |
1 |
Percent of women, ages 18 through 44, with a preventive medical visit in the past year |
2 |
Percent of cesarean deliveries among low-risk first births |
3 |
Percent of very low birth weight (VLBW) infants born in a hospital with a Level III+ Neonatal Intensive Care Unit (NICU) |
4 |
A) Percent of infants who are ever breastfed and B) Percent of infants breastfed exclusively through 6 months |
5 |
A) Percent of infants placed to sleep on their backs, B) Percent of infants placed to sleep on a separate approved sleep surface, C) Percent of infants placed to sleep without soft objects or loose bedding |
6 |
Percent of children, ages 9 through 35 months, who received a developmental screening using a parent-completed screening tool in the past year |
7 |
7.1 Rate of hospitalization for non-fatal injury per 100,000 children, ages 0 through 9; and 7.2 Rate of hospitalization for non-fatal injury per 100,000 adolescents, ages 10 through 19 |
8 |
8.1 Percent of children, ages 6 through 11, who are physically active at least 60 minutes per day; and 8.2 Percent of adolescents, ages 12 through 17, who are physically active at least 60 minutes per day |
9 |
Percent of adolescents, ages 12 through 17, who are bullied or who bully others |
10 |
Percent of adolescents, ages 12 through 17, with a preventive medical visit in the past year |
11 |
Percent of children with and without special health care needs, ages 0 through 17, who have a medical home |
12 |
Percent of adolescents with and without special health care needs, ages 12 through 17, who received services to prepare for the transition to adult health care |
13 |
13.1 Percent of women who had a dental visit during pregnancy; and 13.2 Percent of children, ages 1 through 17, who had a preventive dental visit in the past year |
14 |
14.1 Percent of women who smoke during pregnancy; and 14.2 Percent of children, ages 0 through 17, who live in households where someone smokes |
15 |
Percent of children, ages 0 through 17, who are continuously and adequately insured |
PERFORMANCE MEASURE 1 |
Percent of women, ages 18 through 44, with a preventive medical visit in the past year |
GOAL To increase the percent of women who have an annual preventive medical visit. |
|
|
|
DEFINITION Numerator: Number of women, ages 18 through 44, who report visiting a doctor for a routine checkup in the past year
Denominator: Number of women, ages 18 through 44
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Access to Health Services (AHS) Objective 08: Increase the proportion of adults who receive appropriate evidence-based clinical preventive services. (Baseline: 8.0% in 2015, Target: 10.9%) |
|
|
|
DATA SOURCES Behavioral Risk Factor Surveillance System (BRFSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalPerformanceMeasures |
|
MCH POPULATION DOMAIN Women/Maternal Health
|
|
SIGNIFICANCE An annual well-woman visit provides a critical opportunity to receive recommended clinical preventive services, including screening, counseling, and immunizations, which can lead to appropriate identification, treatment, and prevention of disease to optimize the health of women before, between, and beyond potential pregnancies.1 For example, screening and management of chronic conditions such as diabetes, and counseling to achieve a healthy weight and smoking cessation, can be advanced within a well woman visit to promote women’s health prior to and between pregnancies and improve subsequent maternal and perinatal outcomes.1 The Women’s Preventive Services Initiative (WPSI) is a coalition of national health professional organizations and patient advocates led by the American College of Obstetricians and Gynecologists (ACOG) and works to develop, review, and update recommendations for women’s healthcare preventive services. WPSI recommends an annual well-woman visit beginning in adolescence and continuing across the lifespan with any health care provider offering preventive well-woman care.2
|
|
|
|
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 2 |
Percent of cesarean deliveries among low-risk first births |
GOAL To reduce the percent of cesarean deliveries among low-risk first births. |
|
|
|
DEFINITION Numerator: Number of cesarean deliveries among term (37+ weeks), singleton, vertex births to nulliparous women
Denominator: Number of term (37+ weeks), singleton, vertex births to nulliparous women
Units: 100
Text: Percent
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) Objective 06: Reduce cesarean births among low-risk women with no prior births (Baseline: 25.9% of low-risk females with no prior births had a cesarean birth in 2018, Target: 23.6%) |
|
DATA SOURCES National Vital Statistics System (NVSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalPerformanceMeasures |
|
MCH POPULATION DOMAIN Women/Maternal Health |
|
SIGNIFICANCE Cesarean delivery can be a life-saving procedure for certain medical indications. However, for most low-risk pregnancies, cesarean delivery poses avoidable maternal risks of morbidity and mortality, including hemorrhage, infection, and blood clots—risks that compound with subsequent cesarean deliveries.1 Much of the temporal increase in cesarean delivery (over 50% in the past decade), and wide variation across states, hospitals, and practitioners, can be attributed to first-birth cesareans.1 Moreover, cesarean delivery in low-risk first births may be most amenable to intervention through quality improvement efforts.1 This low-risk cesarean measure, also known as nulliparous term singleton vertex (NTSV) cesarean, is endorsed by the National Quality Forum (#0471) and included within The Joint Commission’s National Quality Measures for hospitals (PC-02), and the Core Set of Maternal and Perinatal Health Measures for Medicaid and CHIP. An Alliance for Innovation on Maternal Health (AIM) patient safety bundle for Safe Reduction of Primary Cesarean Births was released in 2018.2
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 3 |
Percent of very low birth weight (VLBW) infants born in a hospital with a Level III+ Neonatal Intensive Care Unit (NICU) |
GOAL To ensure that higher risk mothers and newborns deliver at appropriate level hospitals.
|
DEFINITION Numerator: Number of VLBW infants born in a hospital with a level III or higher NICU Denominator: Number of VLBW infants (< 1500 grams)
Units: 100
Text: Percent
|
HEALTHY PEOPLE 2030 OBJECTIVE
|
DATA SOURCES Linked birth certificate and hospital data on NICU levels from American Academy of Pediatrics (AAP), CDC Levels of Care Assessment Tool (LOCATe), or state certifications/designations For more detail on possible data sources, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf |
MCH POPULATION DOMAIN Perinatal/Infant Health
|
SIGNIFICANCE Very low birth weight infants (<1,500 grams or 3.25 pounds) are the most fragile newborns with a risk of death over 100 times higher than that of normal birth weight infants (≥2,500 grams or 5.5 pounds).1 VLBW infants are significantly more likely to survive and thrive when born in a facility with a level-III Neonatal Intensive Care Unit (NICU), a subspecialty facility equipped to handle high-risk neonates. In 2012, the AAP provided updated guidelines on the definitions of neonatal levels of care to include Level I (basic care), Level II (specialty care), and Levels III and IV (subspecialty intensive care) based on the availability of appropriate personnel, physical space, equipment, and organization.2 Given overwhelming evidence of improved outcomes, the AAP recommends that VLBW and/or very preterm infants (<32 weeks’ gestation) be born in only level III or IV facilities.2
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see
|
PERFORMANCE MEASURE 4 |
|
|
GOAL To increase the percent of infants who are breastfed and who are breastfed exclusively through six months |
||
|
|
|
DEFINITION Numerators:
Denominators:
Units: 100
Text: Percent |
||
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) Objective 15: Increase the proportion of infants who are breastfed exclusively through 6 months (Baseline: 24.9% of infants born in 2015, Target: 42.4%)
Related to MICH Objective 16: Increase the proportion of infants who are breastfed at 1 year (Baseline: 35.9% of infants born in 2015, Target: 54.1%)
|
||
DATA SOURCES A) National Immunization Survey (NIS) B) National Immunization Survey (NIS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalPerformanceMeasures |
||
MCH POPULATION DOMAIN Perinatal/Infant Health |
||
SIGNIFICANCE The American Academy of Pediatrics (AAP) recommends all infants (including premature and sick newborns) exclusively breastfeed for about six months, followed by continued breastfeeding as complementary foods are introduced for 1 year or longer. Exclusive breastfeeding for six months supports optimal growth and development by providing all required nutrients during that time. Breastfeeding strengthens the immune system, reduces respiratory infections, gastrointestinal illness, and SIDS, and promotes neurodevelopment. Breastfed children may also be less likely to develop diabetes, childhood obesity, and asthma. Maternal benefits include reduced postpartum blood loss due to oxytocin release and possible protective effects against breast and ovarian cancer, diabetes, hypertension, and heart disease.
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
||
PERFORMANCE MEASURE 5 |
|
GOAL To increase the percent of infants placed to sleep on their backs, on a separate approved sleep surface, without soft objects or loose bedding |
DEFINITION Numerators:
Denominators:
Units: 100 Text: Percent |
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 14: Increase the proportion of infants placed to sleep on their backs (Baseline: 78.7% of infants born in 2016; Target: 88.9%);
Related to MICH Objective D3: Increase the proportion of infants who are put to sleep in a safe sleep environment. (Developmental) |
DATA SOURCES Pregnancy Risk Assessment Monitoring System (PRAMS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalPerformanceMeasures |
MCH POPULATION DOMAIN Perinatal/Infant Health |
SIGNIFICANCE Sleep-related infant deaths, also called Sudden Unexpected Infant Deaths (SUID), account for the largest share of infant deaths after the first month of life.1 SUID includes Sudden Infant Death Syndrome (SIDS), ill-defined deaths, and accidental suffocation and strangulation in bed. Due to heightened risk of SIDS when infants are placed to sleep in side (lateral) or stomach (prone) sleep positions, the American Academy of Pediatrics (AAP) has long recommended the back (supine) sleep position. To further reduce SUID, the AAP has expanded recommendations for a safe sleep environment to include, among other practices, using a separate firm sleep surface (eg, crib or bassinet) without soft objects or loose bedding.2
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see
|
PERFORMANCE MEASURE 6 |
Percent of children, ages 9 through 35 months, who received a developmental screening using a parent-completed screening tool in the past year |
GOAL To increase the percent of children who receive a developmental screening. |
|
|
|
DEFINITION Numerator: Number of children, ages 9 through 35 months (2 years), whose parents reported completing a standardized developmental screening questionnaire from a health care provider in the past year with age-specific content on language development and social behavior
Denominator: Number of children, ages 9 through 35 months
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Maternal, Infant, and Child Health (MICH) Objective 17: Increase the proportion of children who receive a developmental screening. (Baseline: 31.1% in 2016-17, Target: 35.8%)
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalPerformanceMeasures |
|
MCH POPULATION DOMAIN Child Health |
|
SIGNIFICANCE Early identification of developmental delays and disabilites is critical to provide referrals to services that can promote health and educational success.1 It is an integral function of the primary care medical home. The American Academy of Pediatrics (AAP) recommends developmental screening at the 9, 18, and 24 or 30 month visit.1 Developmental screening is part of the Core Set of Children’s Health Care Quality Measures for Medicaid and CHIP.
|
|
|
|
EVIDENCE-BASED STRATEGIES
For information about evidence-based strategies related to this measure, see
PERFORMANCE MEASURE 7 |
7.1 Rate of hospitalization for non-fatal injury per 100,000 children, ages 0 through 9
7.2 Rate of hospitalization for non-fatal injury per 100,000 adolescents, ages 10 through 19 |
GOAL To decrease the rate of hospital admissions for non-fatal injury among children ages 0 through 19. |
|
|
|
DEFINITION Numerators: 7.1 Number of hospital admissions with a primary diagnosis of unintentional or intentional injury among children ages 0 through 9 (excludes in-hospital deaths) 7.2 Number of hospital admissions with a primary diagnosis of unintentional or intentional injury among adolescents, ages 10 through 19 (excludes in-hospital deaths)
Denominators: 7.1 Number of children, ages 0 through 9 7.2 Number of adolescents, ages 10 through19
Units: 100,000
Text: Rate |
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Injury and Violence Prevention (IVP) Objective 02: Reduce emergency department (ED) visits for nonfatal injuries. (Baseline: 9,349.5 ED visits per 100,000 population occurred in 2017 (age adjusted to the year 2000 standard population), Target: 7,738.2 ED visits per 100,000 population) |
|
|
|
DATA SOURCES Healthcare Cost and Utilization Project (HCUP) - State Inpatient Database (SID) Population estimates come from the U.S. Census Bureau For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
MCH POPULATION DOMAIN Child Health and/or Adolescent Health |
|
SIGNIFICANCE Unintential injury is the leading cause of child and adolescent mortality, from age 1 through 19.1 Yet for every child death, there are an estimated 25 non-fatal hospitalizations,2 representing a significant source of disability with lifelong mental, physical, and financial impact.1 Effective interventions to reduce injury exist but are not fully implemented in systems of care that serve children and their families.2 Reducing the burden of nonfatal injury can greatly improve the life course trajectory of infants, children, and adolescents resulting in improved quality of life and cost savings. DC. VitalSigns: Child Injury. April 2012. https://www.cdc.gov/vitalsigns/childinjury/
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 8 |
8.1 Percent of children, ages 6 through 11, who are physically active at least 60 minutes per day
8.2 Percent of adolescents, ages 12 through 17 who are physically active at least 60 minutes per day |
GOAL To increase the percent of children and adolescents who are physically active. |
DEFINITION Numerators: 8.1 Number of children, ages 6 through 11, who are reported by a parent to be physically active at least 60 minutes per day in the past week (NSCH) 8.2 Number of adolescents, ages 12 through 17, who are reported by a parent to be physically active at least 60 minutes per day in the past week (NSCH) Number of adolescents in grades 9 through 12 who report being physically active at least 60 minutes per day in the past week (YRBSS)
Denominators: 8.1 Number of children ages 6 through 11 (NSCH) 8.2 Number of adolescents ages 12 through 17 (NSCH) Number of adolescents in grades 9 through 12 (YRBSS)
Units: 100 Text: Percent |
HEALTHY PEOPLE 2030 OBJECTIVE Related to Physical Activity Objective 09: Increase the proportion of children who meet the current aerobic physical activity guideline. (Baseline: 25.9% of children aged 6 to 13 years met the current aerobic physical activity guideline in 2016-17, Target: 30.4%)
Identical (YRBSS) to PA Objective 06: Increase the proportion of adolescents who meet the current aerobic physical activity guideline. (Baseline: 26.1% of students in grades 9 through 12 were physically active for at least 60 minutes on all 7 days of the past week in 2017, Target: 30.6%) |
|
DATA SOURCES National Survey of Children's Health (NSCH); Youth Risk Behavior Surveillance System (YRBSS) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
MCH POPULATION DOMAIN Child Health and/or Adolescent Health |
SIGNIFICANCE Regular physical activity can improve the health and quality of life of Americans of all ages, regardless of the presence of a chronic disease or disability. Physical activity in children and adolescents improves bone health, weight status, cardiorespiratory and cardiometabolic health, and brain health, including improved cognition and reduced depressive symptoms. Physical activity reduces the risk of early life risk factors for cardiovascular disease, hypertension, Type II diabetes, and osteoporosis. In addition to aerobic and muscle-strengthening activities, bone-strengthening activities are especially important for children and young adolescents because the majority of peak bone mass is obtained by the end of adolescence.
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
PERFORMANCE MEASURE 9 |
Percent of adolescents, ages 12 through 17, who are bullied or who bully others |
GOAL To reduce the percent of adolescents who are bullied or who bully others. |
|
DEFINITION Numerators: Number of adolescents in grades 9 through 12 who report that they are bullied on school property or electronically in the past year (YRBSS) Number of adolescents, ages 12 through 17, who are reported by a parent to have been bullied in the past year (NSCH) Number of adolescents, ages 12 through 17, who are reported by a parent to have bullied others in the past year (NSCH)
Denominators: Number of adolescents in grades 9 through 12 (YRBSS) Number of adolescents ages 12 through 17 (NSCH)
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to LGBT Objective 05: Reduce bullying of sexual minority (lesbian, gay, bisexual) high school students. (Baseline: 33.0% in 2017, Target: 25.1%)
Related to LGBT Objective D1: Reduce bullying of transgender students. (Developmental) |
|
|
|
DATA SOURCES Youth Risk Behavior Surveillance System (YRBSS); National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
MCH POPULATION DOMAIN Adolescent Health
|
|
SIGNIFICANCE Bullying, particularly among school-age children, is a major public health problem that is associated with a number of behavioral, emotional, and physical adjustment problems. Adolescents who bully others tend to exhibit other defiant and delinquent behaviors, have poor school performance, be more likely to drop-out of school, and are more likely to bring weapons to school. Victims of bullying tend to report feelings of depression, anxiety, low self-esteem, and isolation; poor school performance; suicidal ideation; and suicide attempts. Bullying victims who also perpetrate bullying (i.e., bully-victims) may exhibit the poorest functioning, in comparison with either victims or bullies. Emotional and behavioral problems experienced by victims, bullies, and bully-victims may continue into adulthood and produce long-term negative outcomes, including low self-esteem and self-worth, depression, antisocial behavior, vandalism, drug use and abuse, criminal behavior, gang membership, and suicidal ideation.
|
|
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 10 |
Percent of adolescents, ages 12 through 17, with a preventive medical visit in the past year |
GOAL To increase the percent of adolescents who have a preventive medical visit. |
|
|
|
DEFINITION Numerator: Number of adolescents, ages 12 through 17, who are reported by a parent to have had a preventive medical check-up with a health care provider in the past year
Denominator: Number of adolescents, ages 12 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Identical to Adolescent Health (AH) Objective 01: Increase the proportion of adolescents who received a preventive health care visit in the past year. (Baseline: 78.7% in 2016-17, Target: 82%) |
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
MCH POPULATION DOMAIN Adolescent Health |
|
SIGNIFICANCE Adolescence is a period of major physical, psychological, and social development. As adolescents move from childhood to adulthood, they assume individual responsibility for health habits, and those who have chronic health problems take on a greater role in managing those conditions. Initiation of risky behaviors, such as unsafe sexual activity, unsafe driving, and substance use, is a critical health issue during adolescence, as adolescents try on adult roles and behaviors. An annual preventive well visit may help adolescents adopt or maintain healthy habits and behaviors, avoid health‐damaging behaviors, manage chronic conditions, and prevent disease. The Bright Futures guidelines recommends that adolescents have an annual checkup from age 11 through 21. The visit should cover a comprehensive set of preventive services, such as a physical examination, immunizations, and discussion of health‐related behaviors including healthy eating, physical activity, substance use, sexual behavior, violence, and motor vehicle safety. The adolescent well-care visit measure for health plans is part of the core measure sets for Medicaid and the National Committee for Quality Assurance. National Adolescent and Young Adult Health Information Center (2016). Summary of Recommended Guidelines for Clinical Preventive Services for Adolescents up to age 18. http://nahic.ucsf.edu/adolescent-guidelines Adolescence is a period of major physical, psychological, and social development. As adolescents move from childhood to adulthood, they assume individual responsibility for health habits, and those who have chronic health problems take on a greater role in managing those conditions. Initiation of risky behaviors, such as unsafe sexual activity, unsafe driving, and substance use, is a critical health issue during adolescence, as adolescents try on adult roles and behaviors. An annual preventive well visit may help adolescents adopt or maintain healthy habits and behaviors, avoid health‐damaging behaviors, manage chronic conditions, and prevent disease. The Bright Futures guidelines recommends that adolescents have an annual checkup from age 11 through 21. The visit should cover a comprehensive set of preventive services, such as a physical examination, immunizations, and discussion of health‐related behaviors including healthy eating, physical activity, substance use, sexual behavior, violence, and motor vehicle safety. The adolescent well-care visit measure for health plans is part of the Core Set of Children’s Health Care Quality Measures for Medicaid and CHIP and the National Committee for Quality Assurance’s Healthcare Effectiveness Data and Information Set. |
|
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 11 |
Percent of children with and without special health care needs, ages 0 through 17, who have a medical home |
GOAL To increase the percent of children with and without special health care needs who have a medical home |
|
|
|
DEFINITION Numerator: Number of children with and without special health care needs, ages 0 through 17, who are reported by a parent to meet the criteria for having a medical home (personal doctor or nurse, usual source for care, family-centered care, referrals if needed, and care coordination if needed)
Denominator: Number of children, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 19: Increase the proportion of children and adolescents who receive care in a medical home. (Baseline: 48.6% in 2016-17, Target: 53.6%) |
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
MCH POPULATION DOMAIN Children with Special Health Care Needs or All Children (CSHCN and non-CSHCN)
|
|
SIGNIFICANCE The American Academy of Pediatrics (AAP) specifies seven qualities essential to medical home care, which include accessible, family-centered, continuous, comprehensive, coordinated, compassionate and culturally effective. Providing comprehensive and coordinated care to children in a medical home is the standard of pediatric practice. Research indicates that children with a stable and continuous source of health care are more likely to receive appropriate preventive care, are less likely to be hospitalized for preventable conditions, and are more likely to be diagnosed early for chronic or disabling conditions.
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
PERFORMANCE MEASURE 12 |
Percent of adolescents with and without special health care needs, ages 12 through 17, who received services to prepare for the transitions to adult health care |
GOAL To increase the percent of adolescents with and without special health care needs who have received services to prepare for the transitions to adult health care. |
DEFINITION Numerator: Number of adolescents with and without special health care needs, ages 12 through 17, who are reported by a parent to have received services to prepare for the transition to adult health care (time alone with a health care provider, active work to gain skills to manage health/health care or understand changes in health care at age 18, discussed shift to adult providers if needed)
Denominator: Number of adolescents, ages 12 through 17
Units: 100 Text: Percent |
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Adolescent Health (AH) Objective R01: Increase the proportion of adolescents (aged 12 to 17 years) with and without special health care needs who receive services to support their transition to adult health care. (Research)
Related to AH Objective 02: Increase the proportion of adolescents who speak privately with a physician or other health care provider during a preventive medical visit. (Baseline: 38.4% in 2016-17, Target: 43.3%) |
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
MCH POPULATION DOMAIN Children with Special Health Care Needs or All Adolescents (CSHCN and non-CSHCN)
|
SIGNIFICANCE The transition of youth to adulthood, including the movement from a child to an adult model of healthcare, has become a priority issue nationwide as evidenced by the 2011 clinical report and algorithm developed jointly by the AAP, American Academy of Family Physicians and American College of Physicians to improve healthcare transitions for all youth and families. Poor health has the potential to impact negatively the youth and young adults’ academic and vocational outcomes. Over 90 percent of children with special health care needs now live to adulthood, but are less likely than their non-disabled peers to complete high school, attend college or to be employed. Health and health care are cited as two of the major barriers to making successful transitions.
|
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
PERFORMANCE MEASURE 13 |
13.1 Percent of women who had a preventive dental visit during pregnancy
13.2 Percent of children, ages 1 through 17, who had a preventive dental visit in the past year |
GOAL 13.1 To increase the number of pregnant women who have a dental visit during pregnancy and 13.2 To increase the number of children, ages 1 through 17, who had a preventive dental visit in the past year. |
DEFINITION Numerators: 13.1 Number of women who report having their teeth cleaned by a dentist or dental hygienist during pregnancy 13.2 Number of children, ages 1 through 17, who are reported by a parent to have seen a dentist or other oral health care provider for preventive dental care in the past year Denominators: 13.1 Number of women with a recent live birth 13.2 Number of children, ages 1 through 17 Units: 100 Text: Percent |
HEALTHY PEOPLE 2030 OBJECTIVE Related to Oral Health (OH) Objective 08: Increase the proportion of children, adolescents, and adults who use the oral health care system. (Baseline: 43.3% in 2016 (age adjusted to the year 2000 standard population), Target: 45.0%) Related to Oral Health (OH) Objective 09. Increase the proportion of low income youth who have a preventive dental visit. (Baseline: 78.8% in 2016-17, Target: 82.7%) |
DATA SOURCES 13.1 Pregnancy Risk Assessment Monitoring System (PRAMS) 13.2 National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
MCH POPULATION DOMAIN Women/Maternal Health, Child Health, and/or Adolescent Heath
|
SIGNIFICANCE Oral health is a vital component of overall health and oral health care remains the greatest unmet health need for children. Insufficient access to oral health care and effective preventive services affects children’s health, education, and ability to prosper. To prevent tooth decay and oral infection, the American Academy of Pediatric Dentistry (AAPD) recommends preventive dental care for all children after the eruption of the first tooth or by 12 months of age, usually at intervals of every 6 months.1 Preventive dental care in pregnancy is also recommended by the American College of Obstetricians and Gynecologists (ACOG) to improve lifelong oral hygiene habits and dietary behavior for women and their families.2
|
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
PERFORMANCE MEASURE 14 |
14.1 Percent of women who smoke during pregnancy
14.2 Percent of children, ages 0 through 17, who live in households where someone smokes |
GOAL 14.1 To decrease the number of women who smoke during pregnancy and 14.2 To decrease the number of households where someone smokes. |
|
DEFINITION Numerator: 14.1 Number of women who report smoking during pregnancy 14.2 14.2 Number of children, ages 0 through 17, who are reported by a parent to live in a household where there is household member who smokes
Denominator: 14.1 Number of live births 14.2 Number of children, ages 0 through 17
Units: 100 Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Maternal, Infant, and Child Health (MICH) Objective 10: Increase abstinence from cigarette smoking among pregnant women. (Baseline: 93.5% in 2018, Target: 95.7%)
Related to Tobacco Use (TU) Objective 15: Increase smoking cessation success during pregnancy among females. (Baseline: 20.2% in 2018, Target 24.4%)
Related to TU Objective 19: Reduce the proportion of children, adolescents and adults exposed to secondhand smoke. (Baseline: 25.5% in 2013-16 (age adjusted to the year 2000 standard population), Target: 17.3%) |
|
|
|
DATA SOURCES and DATA ISSUES 14.1 National Vital Statistics System (NVSS) 14.2 National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures
|
|
MCH POPULATION DOMAIN Women/Maternal Health, Child Health, and/or Adolescent Health
|
|
SIGNIFICANCE Women who smoke during pregnancy are more likely to experience a fetal death or deliver a low birth weight baby. Adverse effects of parental smoking on children have been a clinical and public health concern for decades. Children have an increased frequency of ear infections; acute respiratory illnesses and related hospital admissions during infancy; severe asthma and asthma-related problems; lower respiratory tract infections; and SIDS.
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see Women who smoke during pregnancy are more likely to experience a fetal death or deliver a low birth weight baby. Adverse effects of parental smoking on children have been a clinical and public health concern for decades. Children have an increased frequency of ear infections; acute respiratory illnesses and related hospital admissions during infancy; severe asthma and asthma-related problems; lower respiratory tract infections; and SIDS. The Health Consequences of Smoking—50 Years of Progress. A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. https://www.surgeongeneral.gov/library/reports/50-years-of-progress/index.html |
|
PERFORMANCE MEASURE 15 |
Percent of children, ages 0 through 17, who are continuously and adequately insured |
GOAL To increase the percent of children who are continuously and adequately insured |
|
|
|
DEFINITION Numerator: Number of children, ages 0 through 17, who are reported by a parent to be were continuously insured in the past year with adequate coverage, based on 3 criteria: covers needed services, covers needed providers, and reasonably covers costs.
Denominator: Number of children, ages 0 through 17
Units: 100
Text: Percent |
|
|
|
HEALTHY PEOPLE 2030 OBJECTIVE Related to Access to Health Services (AHS) Objective 01: Increase the proportion of persons with medical insurance. (Baseline: 89.0% in 2018, Target: 92.1%)
|
|
|
|
DATA SOURCES National Survey of Children's Health (NSCH) For details about data source methodology, SAS code, national and states estimates, standard errors, stratifiers, and data alerts, see https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf
For national and state trends and data notes, see https://mchb.tvisdata.hrsa.gov/PrioritiesAndMeasures/NationalOutcomeMeasures |
|
MCH POPULATION DOMAIN Child Health, Adolescent Health, and/or Children with Special Health Care Needs
|
|
SIGNIFICANCE Inadequately insured children are more likely to have delayed or forgone care and are less likely to have a medical home and receive needed referrals, care coordination, and family-centered care.1 The American Academy of Pediatrics (AAP) highlighted the importance of this issue with a policy statement. The major problems cited were cost-sharing requirements that are too high, benefit limitations, and inadequate coverage of needed services.2
(1) Kogan MD, Newacheck PW, Blumberg SJ, Ghandour RM, Singh GK, Strickland BB, van Dyck PC. Underinsurance among children in the United States. N Engl J Med. 2010 Aug 26;363(9):841-51. http://www.nejm.org/doi/full/10.1056/NEJMsa0909994
(2) Hudak ML, Helm ME, White PH, Committee on Child Health Financing. Principles of Health Care Financing. Pediatrics. 2017; 140 (3) w20172098. https://pediatrics.aappublications.org/content/140/3/e20172098 Kogan MD, Newacheck PW, Blumberg SJ, Ghandour RM, Singh GK, Strickland BB, van Dyck PC. Underinsurance among children in the United States. N Engl J Med. 2010Aug 26;363(9):841-51. http://www.nejm.org/doi/full/10.1056/NEJMsa0909994
EVIDENCE-BASED STRATEGIES For information about evidence-based strategies related to this measure, see |
|
APPENDIX D: FAMILY PARTNERSHIP CONTINUUM
Family partnership is defined as patients, families, their representatives, and health professionals working in active partnership at various levels across the health care system—direct care, organizational design and governance, and policy making—to improve health and health care. This partnership is accomplished through the intentional practice of working with families for the ultimate goal of positive outcomes in all areas through the life course.3 The Figure below represents a continuum of engagement with families and individuals at different levels in the health care system, from the consultation, involvement, and partnership stage.4 Additionally, the Family Engagement in Systems Assessment Tool (FESAT) and Toolkit, developed by Family Voices, assesses patient and family engagement at the systems level. The Toolkit also provides activities to support and improve systems-level activities with families. To access, click here: https://familyvoices.org/familyengagementtoolkit/
A
Multidimensional Framework for Patient and Family Engagement in
Health and Health Care
|
|
|||||
Levels of Engagement |
|
Consultation |
|
Involvement |
|
Partnership and Shared Leadership |
Direct Care |
|
Patient receive information about a diagnosis |
|
Patients are asked about their preferences in treatment plan |
|
Treatment decisions are made based on patients’ preferences, medical evidence, and clinical judgement |
|
|
|
|
|
|
|
Organizational Design and Governance |
|
Organization surveys patients about their care experiences |
|
Hospital involves patients as advisers or advisory council members |
|
Patients co-lead hospital safety and quality improvement committees |
|
|
|
|
|
|
|
Policy Making |
|
Public agency conducts focus groups with patients to ask opinions about a health care issue |
|
Patients’ recommendations about research priorities are used by public agency to make funding decisions |
|
Patients have equal representation on agency committee that makes decisions about how to allocate resources to health programs |
|
|
|
|
|
|
|
|
Factors influencing engagement:
|
|||||
 Continuum
of Engagement
Continuum
of Engagement







APPENDIX E: |
NEEDS ASSESSMENT − BACKGROUND AND CONCEPTUAL FRAMEWORK
|
Conducting a Needs Assessment is a systematic process to acquire an accurate, thorough picture of the strengths and weaknesses of a state’s public health system that can be used in response to the preventive and primary care services needs for ALL pregnant women, mothers, infants (up to age one), and children, including children with special health care needs
[Section 505 (a)(1)]. The Needs Assessment process includes the collection and examination of information about the state’s capacity and infrastructure, needs and desired outcomes for the MCH population, and legislative mandates, etc. This information is utilized to determine priority goals, develop a plan of action, and to allocate funds and resources. The Needs Assessment is a collaborative process that should include the HRSA/MCHB, the state Department of Health, families, practitioners, the community, and other agencies and organizations within each state and jurisdiction that have an interest in the well-being of the MCH population.
Title V of the Social Security Act requires states to conduct a statewide Needs Assessment every five years. States will report on the next Five-year Needs Assessment in calendar year 2020 as part of the FY 2021 MCH Block Grant Application process. Rather than submitting a comprehensive “stand-alone document”, as was required prior to 2015, states now submit a Five-Year Needs Assessment Summary that concisely describes the process and findings. As the Needs Assessment document may serve multiple purposes, a state may wish to develop a more comprehensive document to meets its broader needs. This document cannot be submitted in place of the required Five-year Needs Assessment Summary, but states may include a URL, if the document is posted online, in the Five-year Needs Assessment Summary or they may submit the document as an attachment to the Application/Annual Report in the electronic application system. Over the five-year reporting period, states are encouraged to continuously revisit the Five-Year Needs Assessment Summary and to provide updates, as needed, in the interim year Applications/Annual Reports. Furthermore, it is expected that states will have ongoing communication with stakeholders and partners throughout the Needs Assessment process and continue to engage with such partners during the interim reporting years.
The primary goal of the statewide Needs Assessment is to improve MCH outcomes and to strengthen its state, local and community partnerships for addressing the needs of its MCH population. The following figure illustrates the continuity of the Needs Assessment process and its relationship to the planning and monitoring functions of Title V and the population that it serves.

State MCH Block Grant Needs Assessment, Planning, Implementation and Monitoring Process

A brief description of the steps involved in the Public Health Planning Cycle to inform ongoing needs assessment is presented in the following sections.
Engage Stakeholders
As depicted, the starting point for the Needs Assessment process is to engage stakeholders. Engaging stakeholders and strengthening partnerships is a continuous and on-going activity. The state needs strong partnerships with its stakeholders throughout the Needs Assessment process. Effective coalitions can help the state to realistically assess needs and identify desired outcomes and mandates, assess strengths and examine capacity, select priorities, seek resources, set performance objectives, develop an action plan, allocate resources, and monitor progress for impact on targeted outcomes.
Assess Needs and Identify Desired Outcomes and Mandates
The second stage in the process is to assess needs of the MCH population groups using the Title V National Outcome Measures (NOMs), national, state and strategy performance measures and other available state-level quantitative and qualitative data. States should assess MCH population needs based on the following five population health domains: 1) Women/Maternal Health; 2) Perinatal/Infant Health; 3) Child Health; 4) Adolescent Health; and 5) Children with Special Health Care Needs (CSHCN). These population health domains fall with the three MCH population groups that are defined in Section 505(a)(1) of the Title V legislation. The anticipated outcome of this assessment is to identify community/system needs and desired outcomes by specific MCH population groups. In addition, the state will need to identify needs and desired outcomes for cross-cutting and systems issues. The state will also need to identify legislative, political, community-driven, financial, and/or other internal and external mandates which may go beyond the findings identified through the Needs Assessment process but are priorities for implementation within the state.
Examine Strengths and Capacity
The third stage in the Needs Assessment process is examining strengths and capacity. This stage involves examining the state’s capacity to engage in various activities, including conducting the statewide Five-year Needs Assessment and collecting/reporting annual performance data based on the five identified MCH population health domains and the types of MCH services provided.
This stage involves describing and assessing the state’s current resources, activities, and services as well as the state’s ability to continue to provide quality services by each of the three MCH service levels. These levels include 1) Direct Services; 2) Enabling Services; and 3) Public Health Services and Systems. The anticipated outcome is a better understanding of the relationship of the state’s existing program/system capacity to its identified strengths and needs. This examination may reveal strengths and weaknesses in capacity not previously identified.
Select Priorities
In the select priorities stage, each state examines the identified needs and matches them to the desired outcomes, required mandates and level of existing capacity. As a result, states will select seven to ten priority areas for targeted focus in promoting continued improvement and progress. Examples of inputs include: the Needs Assessment process, the opinions of stakeholders, the examination of program capacity and the political priorities within the state. The anticipated outcome is the development of a set of priority needs (between seven and ten), which are unique to the individual state based on its Needs Assessment findings. Priorities identified should address areas in which the state believes there is reasonable opportunity for a focused programmatic effort (e.g., new or enhanced interventions, initiatives, or systems of care) to lead to an improved outcome.
Set Performance Objectives
Setting performance objectives consists of two phases. In the first phase, each state will develop action strategies to address their identified priority needs. Based on the priority needs and program strategies developed, the state will select five National Performance Measures (NPMs), Evidence-based or –informed Strategy Measures (ESMs) for addressing each of the selected NPMs, and State Performance Measures (SPMs). SPMs should be based on the state’s identified MCH priorities and target those priority needs that are not fully addressed by the selected NPMs and their related ESMs.
Secondly, the state will set five-year targets (i.e., performance objectives) for the five selected NPMs, the ESMs and the SPMs. The anticipated results of this stage are the identification of NOMs, NPMs, ESMs and SPMs that directly relate to the state priorities and establish a level of accountability for achieving measureable progress.
Develop an Action Plan
The next stage is to develop an action plan, which involves the planning and identification of specific activities for implementing the program strategies which were developed in Stage 5 to address the identified priority needs and selected national/state measures. In developing an Action Plan, states will create the Five-year State Action Plan Table.
In developing the Action Plan, the state shall complete the Five-year State Action Plan Table as part of the first year Application/Annual Report in the five year cycle. This Table is a tool to assist states in aligning their program strategies, NPMs, SPMs and ESMs with the priority needs that were identified in the Five-year Needs Assessment. Updates to the strategies, activities and measures will be provided by the state, as needed, in subsequent interim year Applications/Annual Reports.
Figure 4 in Part Two, Section II of the Application/Annual Report Guidance depicts the steps involved in the development of, and the annual reporting on, the implementation of the Five-year State Action Plan.
Seek and Allocate Resources
Following the identification of program activities is the allocation of resources stage. In this stage, the focus is on the funding of planned activities to address state priorities. Inputs include the five-year State Action Plan, current budgets, political priorities, and partnerships. The anticipated outcome is the development of a program budget and plan that directs available resources towards the activities identified in Stage Six as the most important for addressing the state's priorities.
Monitor Progress for Impact on Outcomes
In monitoring progress for impact on outcomes, the states examine the results of their efforts to see if there has been improvement. Inputs include NOMs, NPMs, SPMs and ESMs, performance objectives and other quantitative and qualitative information. Potential outcomes may include altered activities and shifting of resource allocations to address current levels of performance and availability of resources. Feedback loops between various stages of the process allow for continuous input and re-evaluation of the outputs.
Report Back to Stakeholders
This final step assures accountability to the stakeholders and partners who have worked with the MCH staff throughout the Needs Assessment process. It also assures the continued involvement of all stakeholders and partners in the ongoing Needs Assessment processes.
APPENDIX F: ASSURANCES AND CERTIFICATIONS

APPENDIX G: |
REQUIRED APPLICATION/ANNUAL REPORT COMPONENTS AND TIMELINE
|
Submission Date |
Application Year |
Annual Report Year |
July 15, 2021 |
Fiscal Year (FY) 2022 (Year 02 Application of Five-Year Reporting Cycle.)
|
FY 2020 (Year 05 of Previous Reporting Cycle)
|
July 15, 2022 |
FY 2023 (Year 03 Application of Five-Year Reporting Cycle)
FY 2023 (Continued)
|
FY 2021 (Year 01 of Five-Year Reporting Cycle)
FY 2021 (Continued)
|
July 17, 2023 |
Fiscal Year (FY) 2024 (Year 04 Application of Five-year Reporting Cycle.)
|
FY 2022 (Year 02 of Five-Year Reporting Cycle)
|
APPENDIX H: |
FINANCIAL BUDGET AND EXPENDITURE REPORTING
|
Importance of Financial Reporting
As a federal grant, the Title V Maternal and Child Health (MCH) Services Block Grant to States Program requires financial and programmatic reporting to demonstrate accountability in the use of federal funds. Consistent with the intent of a formula block grant, the financial reporting of a state’s planned budget for the Application year and the expenditures for the Annual Report year in the MCH Block Grant is defined at a high level for financial data collection. The intent of this financial reporting is to demonstrate how both federal and non-federal resources advance the Federal-State Partnership and support state-led efforts to develop and implement a five-year State Action Plan that responds to its identified MCH priority needs.
Financial reporting is required in the Financial Narrative and Forms 2, 3a, and 3b, as well as related Form 5. The line items on Forms 2, 3 and 5 are mandated in the legislation. Instructions for completing these reporting forms are attached to the individual reporting form. The purpose of this appendix is to provide supportive discussion on how the financial forms and the individuals served work in tandem to tell the state’s Title V story.
The Financial Forms
There are five forms related to financial and related programmatic reporting that are to be completed in each year’s submission of the MCH Block Grant Application/Annual Report. These forms are:
SF-424 – Application Financial Assistance. This is a federal form that officially requests the application year funding from the federal government. This form is used by HRSA Grants Management for initiating funding to the state.
Form 2 – MCH Budget/Expenditure Details, which breaks out the Application year budget and Annual Report year expenditures by source of funding. Both budget and expenditures include administrative costs.
Form 3a – Budget and Expenditure Details by Types of Individuals Served, which breaks out funding by MCH populations (pregnant women, infants <1, children 1 through 21 years, children with special health care needs [CSHCN], and all others). The budget and expenditures by individuals served are broken out by the federal and non-federal allocation, besides being further broken down by population. It is important to note that the reporting on this form does NOT include administrative costs.
Form 3b - Budget and Expenditure Details by Types of Services, which breaks out funding by the three MCH Pyramid (Figure 1) service categories (direct services, enabling service, and public health services and systems). Like Form 3a, the budget and expenditures by types of services are broken out by the federal and non-federal allocation, besides being further broken down by types of services. There is additional detailed reporting for direct services by population, and for expenditures of direct services, by specific types of direct services. It is important to note that, like Form 2, Form 3b also should include administrative costs.
Form 5a Count of Individuals Served By Title V, and Form 5b, Total Percentage of Population Served by Title V, which documents the populations served by total Federal-State Partnership Funding. Form 5a reports those who received a direct or enabling service funded by Title V in each of the MCH population groups, while the state provides an estimate for the total percentage of populations who received a Title V-supported service in each of the MCH population groups across all levels of the MCH Pyramid, including public health services and systems on Form 5b. Total expenditures provided by population served for the reporting year on Form 3a should relate to the estimate of all MCH populations reached on Form 5.
How the Financial Reporting Forms are Connected
In order to understand how the finances are planned and support the work of the Federal-State Title V Partnership, there needs to be an understanding of four major financial questions that underpin the Title V MCH Services Block Grant:
What is the source of funding? (Form 2)
How are the funds distributed across MCH population groups? (Form 3a)
What types of services are planned and supported with the funding? (Form 3b)
4. What is the reach of these funds across population groups? (Form 5)
The combination of these four questions provides a broad understanding of how Title V funds support the work of the state Title V program and its activities to reach its MCH populations.
The source of funding has strict legislative financial requirements that include a state match to receive the federal allocation. As for the federal allocation, Section 503(a) requires that the Secretary make payments “for each quarter, of an amount equal to four-sevenths of the total of the sums expended by the State during such quarter in carrying out the provisions of this title.” This provision means that three-sevenths is provided by the state. In short, states must provide a three dollar match for every four federal dollars allocated. The state must also maintain the state funding at a level at least equal to the level provided in 1989 to address the requirement for the maintenance of effort [Section 505(a)(4)].
The federal allocation has certain characteristics. The federal allocation to the 59 states and jurisdictions is based on a legislative formula that considers in part the number of children in poverty in a state compared to the total number of children in poverty nationally. Also, both the budget and expenditures for this federal allocation must meet the requirement of “30/30/10” (i.e., at least 30% of the budget/expenditures must be for primary and preventive services for children, at least 30% of the budget/expenditures must be for children with special health care needs, and no more than 10% can be planned/expended on administrative costs). Once the level of federal and state funding is determined, each state decides how those resources will be allocated across the MCH populations and distributed to support a range of MCH program activities. This discretion in determining how to best invest federal Title V funds to most effectively complement state-supported efforts in addressing the unique needs of each individual state is key to understanding how the MCH Block Grant program is administered. Each state has unique needs, which are reflected in the development and implementation of a Five-Year State Action Plan (SAP) to assure the delivery of needed services to its MCH population.
Relationship Between Form 2 and Form 3
States report federal and non-federal budget and expenditures on Form 3a and 3b separately, which provides the opportunity to assure that reporting in the three areas of interest (i.e., funding by source, individuals served, and types of services) is consistent across the forms. There are several specific areas across which accurate reporting is needed to assure that the budget and expenditures reported on each of the forms are correct, and the Title V Information System (TVIS) has been programmed with validations across forms to help guide accurate reporting.
Specifically, the state should consider the following concepts to assure accuracy in its reporting across Forms 2, 3a, and 3b:
Form 2 Federal Allocation Requirements:
Form 2, Line 1A: Federal Allocation for Preventive and Primary Care for Children. At least 30% of the Federal Allocation for both budget and expenditures should be entered.
Form 2, Line 1B: Federal Allocation for Children with Special Health Care Needs. At least 30% of the Federal Allocation for both budget and expenditures should be entered.
Form 2, Line 1C: Federal Allocation for Title V Administrative Costs. No more than 10% for administrative costs should be entered.
Form 2, Line 2: Federal Allocation Subtotal of Lines 1A-C for Children, Children with Special Health Care Needs, and Administrative Costs. This amount does not have to equal 100%, as it does not include pregnant women and all others.
Form 2, Line 7: Total State Match. This amount must meet or exceed the FY1989 Maintenance of Effort on Line 7A, and must meet the state match requirement, as described above.
Since Form 3a is broken out by federal and non-federal allocations by population, those specific populations that require a certain level of federal support on Form 2 (children and children with special health care needs) must agree with those same populations on Form 3a for the federal allocation.
Form 2, Line 1A and Form 3a, Line 1A.3: Federal Allocation for Children. The federal funding provided must agree for both budget and expenditures on these two forms.
Form 2, Line 1B and Form 3a, Line 1A.4: Federal Allocation for Children with Special Health Care Needs. The federal funding provided must agree for both budget and expenditures on these two forms.
Form 3b: Breaking out Types of Services and Defining Types of Direct Services in Detail
The Title V MCH Services Block Grant serves as a major source of funding supporting the MCH public health system and may also serve as a payer of last resort in many states. Understanding the extent to which services are supported by both federal allocation and the state match is key to understanding the fiscal and health services environment in which Title V operates and better tells the state Title V story about the services delivered. Form 3b captures these data, and one area of reporting of particular interest on Form 3b is the reporting on direct services, which is broken out by MCH populations and further detailed on the specific type of direct services. The state should report as much detail as possible on Form 3b, Line 4 on the types of direct services, as this reporting helps provide a context on Title V’s ongoing role in the health service environment in the state.
Effective financial reporting on the financial forms requires clear understanding of how the funding is distributed and used from the source of funding and the types of services provided to which MCH population. The description of how the financial data reported on these forms work is outlined in detail in Financial Narrative for Expenditures section (pages 27 – 28) of the Title V MCH Block Grant Application/Annual Report Guidance. The state “should reflect on the federal and non-federal monies that have been obligated and spent. This discussion is intended to provide the reader with an understanding of how the supported programs and services link with the state’s MCH priority needs and meet the requirements of Title V legislation.”
Form 5b: Population Estimates Reported are Linked to Allocations Reported on Form 3a
Data estimates reported on the MCH population reached on Form 5b are closely linked with the expenditures reported for each MCH population on Form 3a, since the total support noted with both the federal and non-federal allocations would be the supporting the MCH populations reported on Form 5b with services. As the state provides the financial data on its reporting forms, recognizing the reach of the allocations to the population served is necessary for accurate reporting.
Use of Notes on the Forms versus Reporting in the Financial Narrative
Whenever financial data are provided on Forms 2, 3a, and 3b and there may be a need for clarification on what is being reported, a state is encouraged to use the note feature in TVIS to explain the data. This note feature should be used to explain significant differences (10% or more) between the budget and the expenditures, details on the types of programs and activities associated with a specific financial figure that needs explanation, or any other pertinent information about the reported financial data. It is a judgment call if the reporting is better in a note or the Financial Narrative or both. A guiding rule is that if it is a high-level report of how the program operates, it should be in the Financial Narrative, while a more specific explanation for a number being reported would be better captured in a field or form-level note.
Financial Narrative Reporting
In the Financial Narrative, the state provides a budget plan for the Application year and reports on its expenditures for the Annual Report year. This narrative around the Annual Report year expenditures is a reflection on how the federal and state allocations are being utilized to support the implementation of a state’s Five-Year Action Plan and includes a comparison of planned, budgeted activities with actual expenditures for that fiscal year. The state should link the allocation of financial resources with outcomes achieved relative to the State’s Title V program plan, which provides the reader with an understanding of the reach of the state Title V program activities to its MCH populations.
Connecting the Financial Forms to the State Action Plan Narrative
States are encouraged to think strategically about how well the information reported through the financial forms supports and connects to the State Action Plan narrative. Three examples are provided on the following page to assist states in assuring that the financial forms and the narrative discussion tell a consistent and cohesive story on the role of Title V in the state.
Example
3 – A state
that relies heavily on partnerships to provide funding and support
for key MCH initiatives:
When a
state’s financial forms reflect limited availability of Title
V partnership funds, the narrative would be expected to describe a
more limited scope of Title V strategies, and/or leveraging of
partners to address key MCH needs.
Example
1 – A State with strong support for public health
infrastructure:
When
a state’s financial forms reflect heavy investment in public
health infrastructure, the narrative would be expected to speak of
key public health strategies that are designed to address MCH
priority needs.
A state selects NPM #11 for the Child Health Domain, which is an
optional target population. In selecting this measure, the state
must also address the CSHCN Domain. The state may choose to count
this measure in either the CSHCN Domain or the Child Health Domain.
If selected as the NPM for the Child Health Domain, the state must
select a second NPM from the CSHCN Domain.
Example
2 – A State with
high levels of state match that support direct services for CSHCN:
When
a state’s financial forms reflect high levels of state match
to support direct services, the strategies should describe the role
that Title V plays in supporting these services.
APPENDIX I: |
POPULATION HEALTH & CHILDREN WITH SPECIAL HEALTH CARE NEEDS (CSHCN)5 |
Rationale for CSHCN Population Health Strategies
Children and youth with special health care needs6 need enhanced access to high quality, comprehensive health care in well-integrated, community-based systems due to the complex nature of their health and social conditions. Even if these services are available, they are often not well coordinated across multiple service systems. CSHCN and their families should receive services and supports through a comprehensive system to achieve optimal health and quality of life.7 To increase reach, impact, and sustainability of federal/state funds, State Title V programs are encouraged to incorporate public health services, systems, or population health strategies. Promoting the effective and efficient organization and utilization of resources to assure access to necessary comprehensive services for CSHCN8 and their families require State Title V efforts to strengthen the systems that serve this population and the policies that influence and guide these systems.
Definition: Population Health Strategies for CSHCN
A population health strategy for CSHCN intends to improve the health and well-being of an entire group or subgroup.910 These strategies occur at the policy11 or systems12 level and are measurable over time. They are designed to improve health equity and often focus on social and environmental factors.
Why implement strategies at the policy and systems level?
CSHCN and their families face substantial barriers to health care. The following 2017-2018 National Survey of Children’s Health results13 demonstrate the inequities CSHCN and their families experience around access to care issues and the compounding effects of social determinants of health across systems that serve this population.
Nearly one in five (18.5%) children and youth younger than 18 years in the U.S. have a special health care need.
White children were more likely (21.3%) to receive care within a well-functioning system than Black (13.7%), Hispanic (13.2%), or Asian (13.5%) children.
33% of CSHCN experience two or more adverse childhood events compared to 15% of children without a special health care need.
CSHCN with a household income below federal poverty level were significantly less likely to have a medical home. More than half of CSHCN (57%) do not receive care that meets medical home criteria; nearly one-third (30%) of those who need care coordination did not receive it.
CSHCN were significantly more likely to live in households that could not always afford to eat good nutritious meals than non-CSHCN. Among CSHCN, those with more complex needs were significantly more likely than those with less complex needs.
Almost three times as many families of CSHCN were frustrated in their efforts to get services for their child compared to families of non-CSHCN (36% vs 13% respectively).
One-third (34%) of all children received developmental screening.
More than 80% of CSHCN ages 12 through 17 years do not receive services necessary for transition to adult health care.
Examples of State Title V Programs Implementing Population Health Strategies
There is not one correct way to implement a population health strategy for CSHCN and families. Additionally, population health approaches may be developed and implemented incrementally to reach an entire CSHCN population. The examples below illustrate various population health approaches a state Title V program can take to implement policy and systems change.
Population based approach reaching MCH population, where CSHCN are a subset: Building capacity of healthcare professionals to address social determinants of health (RI) |
Need: To improve the social determinants of health for the state’s maternal and child health population.
Goal: The state’s goal was to sustain and build the capacity of non-licensed health care professionals to address the social, environmental, and economic determinants of health.
Mechanism/Strategy for Change: The state developed peer-to-peer support networks within the healthcare system. Such networks include CSHCN parent consultants, community health workers (CHW), and peer resource specialists. The state developed mechanisms to certify CHW, build the capacity of CHW, and convene multi-payer Community Health Teams. State Title V funds are used to pay for some positions, but not services rendered. The intention of this initiative is to reach all MCH populations in the state; it includes specific training for personnel to ensure that CSHCN and their families benefit equally from the services.
Intended Audience/Population: Entire MCH population in the state, where CSHCN are addressed as a subset deserving special attention.
Measurement and Outcomes: The state is currently collecting process data on the number of CHW certified. The intention is to collect outcome data on quality of life for CSHCN and families, and the percent of families who report increased access to supports and services.
Population Health Characteristics: This is an example of how Federal and state Title V resources can be leveraged with existing efforts across other sectors and programs to advance systems that serve CSHCN and their families to impact a greater proportion of the population. |
Population based approach reaching entire state CSHCN population: Transforming the system of health care to focus on quality of life for CSHCN and their families (FL) |
Need: Health care delivery is increasingly influenced by quality measures. Commonly used metrics for children focus on immunizations and well child care visits, which are important but insufficient for CSHCN who have many complex health needs.
Goal: The state’s goal was to modify the use of quality measures to better reflect what is important to CSHCN and their families.
Mechanism/Strategy for Change: The state’s Title V program, under the authority of the state surgeon general, convened a technical advisory panel composed of youth with special health care needs, families of CSHCN, clinicians, insurers, agency leaders, and experts in quality measurement. The panel recommended that quality of life measures, for both children/youth and their caregivers, be included in health insurance programs and in Title V programs for CSHCN. These recommendations were implemented for all Title V programs and for the state health insurance program for CSHCN.
Intended Audience/Population: All CSHCN and their families in the state.
Measurement and Outcomes: Data from quality of life measures for both CSHCN and their caregivers are being collected by organizations contracted to provide Title V CSHCN services and by the state managed care organization, which insures over 70,000 CSHCN. This program began in 2019, data are not yet available. The next steps will be to analyze whether quality of life measures correlate with health care experiences (e.g. hospitalizations, unmet health care needs, etc.) and whether health care plans and providers and improve quality of life measures.
Population Health Characteristics: This is an example of how Federal and state Title V funds can be used to influence the system of services for CSHCN and their families. If collecting data on quality of life is successful for the state managed care plan, the next step will be to work with the state Medicaid office to extend the program to all managed care plans that include CSHCN. This movement towards policy and systems level change happens incrementally and can lead to measurable population outcomes. |
Population based approach reaching entire state CSHCN population: Ensuring the system of services for CSHCN and families through telemedicine (CO) |
Need: Families of CSHCN in the rural areas of the state report barriers to accessing specialty care, specifically traveling long distances, difficulty transporting children with complex needs and missed work time.
Goal: The state’s goal was to improve access to pediatric specialty care, with a focus on rural and remote geographic locations, by implementing telemedicine statewide.
Mechanism/Strategy for Change: The state transitioned Title V funded clinics to a children’s hospital and contracted with the hospital to expand the use of telemedicine for rural regions and improve access to various types of pediatric specialists.
Intended Audience/Population: CSHCN and their families, primary and specialty providers in rural areas of Colorado, hospital-based pediatric specialists and local public health agencies.
Measurement and Outcomes: Families report improved access to care and quality of life (time to get care, proximity of care, faster response to changes in symptoms, fewer missed days of work). The shift contributed to state level policy changes around use and reimbursement of telemedicine. This example includes process indicators used to show progress: number of clinics utilizing telemedicine for specialty care (including behavioral health), number of specialty areas accessible via telemedicine, percent of families reporting fewer trips to the children’s hospital.
Population Health Characteristics: Although many stakeholders, especially clinicians and youth/families, focus on providing health care services to individuals, the state Title V program is best positioned to examine the system as a whole. This is an example of how the state Title V program understood that a partner was better positioned to provide direct, outreach services. By transferring these clinics, Title V was able to redirect resources to improve the overall system and increase access to pediatric care for all CSHCN in the state, versus only individuals served through the Title V-funded outreach clinics. Through the contract with the children’s hospital, Title V was able to influence an increased focus on the more rural areas of the state where CSHCN experienced disparities in access and quality of care. |
Population based approach reaching subset of CSHCN (Young Adults with Medical Complexity (YAMC): Pilot Intended to Develop into A Population Based Approach (OR) |
Need: Young adults with medical complexity (YAMC) are not adequately prepared for, or supported in, the transfer of care from pediatric to adult primary care.
Goal: The state’s goal is to provide support to YAMC and/or their families to identify and establish care with an adult primary care provider (PCP).
Mechanism/Strategy for Change: The state convened a team composed of family representatives, clinical providers, and Title V CSHCN staff to develop, test and revise a multi-stage strategy to (a) alert YAMC and their families that an adult primary care provider is needed, (b) create a Health Passport (a.k.a., essential care plan information) to share with an adult provider, (c) review insurance plan and other key characteristics of potential adult providers, and (d) schedule and attend an appointment with an adult PCP. The state’s plan is that through quality improvement practice, we will identify a strategy(ies) that can be spread over time to health systems throughout Oregon to support the entire population of YAMC.
Intended Audience/Population: Young adults ages 17 years and older who meet the Complex Chronic Disease category of the Pediatric Medical Complexity Algorithm (PMCA; Simon et al., 2014) and do not yet have an adult primary care physician. Because the state is developing and piloting a strategy using quality improvement methodology, the project’s initial focus is on youth who meet the age and complexity criteria and who receive primary care through Oregon Health & Science University (OHSU) pediatric clinics.
Measurement and Outcomes: The state intends to (1) reduce the amount of time families spend attempting to identify an adult provider, (2) confirm that the YAMC established with an adult PCP, (3) observe increases in use of primary care by this population, and (4) observe decreases in emergency room use for this population. Although the state’s strategy is in a developmental phase, the current process outcomes are: (1) clinic staff time dedicated to strategy implementation, (2) strategy acceptability to clinic staff and families/YAMC, (3) enrollee attendance at transfer preparation appointments, and (4) completion of Health Passports for each enrolled YAMC.
Population Health Characteristics: This provides an example of how population health approaches may start as a pilot project or smaller initiative with a subgroup of the population. Title V programs use a variety of mechanisms, e.g., quality improvement and Implementation Science Frameworks, to develop, implement, test, improve, and scale-up pilot projects or initiatives to reach a broader population. Through quality improvement practice, the state will identify a strategy(ies) that can be spread over time to health systems throughout Oregon to support the entire population of YAMC. |
Population based approach reaching subset of CSHCN (Latino CSHCN): Improving care coordination for CSHCN and families through standardized training (Generic example) |
Need: Latino/Hispanic CSHCN and their families are less likely to receive care in a well-functioning system than White CSHCN and their families.
Goal: The state’s goal was to improve the quality and effectiveness of care coordination services for Latino CSHCN and families by implementing a standardized Care Coordination Curriculum.
Mechanism/Strategy for Change: The state developed a culturally responsive Care Coordination Curriculum in partnership with the Coalition of Latino Communities, a statewide advocacy organization. The state and Coalition piloted the curriculum with ACO and clinic care coordinators in three regions. After monitoring adherence to the model for 6 months, obtaining user feedback, and making curriculum adjustments, Title V and Coalition staff conducted Care Coordination Curriculum trainings in the remaining four regions. The final implementation phase of this strategy entailed collaborating with Medicaid to reimburse for care coordination services. Additionally, the state required that all care coordinators who serve CSHCN and their families through FQHCs to be trained using the curriculum.
Intended Audience/Population: All Medicaid-insured Latino CSHCN and their families in the state.
Measurement and Outcomes: The state began collecting process data describing the number of care coordinators trained and the number of care coordinators adhering to the curriculum. Additionally, the state collected outcome data to capture family satisfaction and quality of life at baseline and after one year of implementation in all regions. The state also tracked change over time in the percent of Latino CSHCN and families that report receiving effective care coordination services through the National Survey of Children’s Health.
Population Health Characteristics: This is an example of how movement towards policy and systems level change happens incrementally and leads to measurable population outcomes, as indicated by the satisfaction and quality of life measures collected in this example. |
APPENDIX J: |
MCH Workforce Capacity
|
The health of the nation’s women, children, youth, and families is influenced by a wide array of factors. At the foundation of a healthy community is a highly qualified, diverse workforce that can positively affect maternal and child health at the individual, community, and policy levels14. Successful implementation of the five-year State Action Plan requires a workforce that is adequate in size, effectively trained and properly supported. State Title V programs have an important role in the ongoing assessment of MCH staff competencies and training needs, identification of skill and technical gaps, and provision of professional development and growth opportunities for staff to help assure optimal impact for state Title V MCH programs. Regular and systematic assessment of the MCH public health workforce can lead to improved knowledge, competence and effectiveness of the MCH workforce, and also support staff recruitment and retention in Title V.
There are several tools available to state Title V agencies to assist in assessing the training and professional development needs of staff and in identifying learning opportunities. The following resources outline critical skills important to fostering a highly skilled and qualified MCH public health workforce and link to resources tailored to the professional development of state Title V staff.
MCH Leadership Competencies https://mchb.hrsa.gov/training/documents/MCH_Leadership_Competencies_v4.pdf
MCHB in partnership with stakeholders developed the MCH Leadership Competencies in order to support current and future MCH leaders by defining the knowledge and skills necessary to lead in MCH. The MCH Leadership Competencies describe the necessary knowledge, skills (foundational and advanced), personal characteristics, and values within a framework designed to support and promote MCH leadership. The Competencies can be used in a variety of ways, including:
As a framework to identify the knowledge and skills needed to develop current and future Title V leaders.
To cultivate, sustain, grow, and measure leadership within the current MCH workforce, including new and seasoned Title V staff and leaders.
To guide measurement and evaluation of leadership training for Title V staff.
MCH Self-Assessment Tool
https://www.mchnavigator.org/assessment/
The
MCH Self-Assessment is an online tool aligned to the MCH Leadership
Competencies that can be used to identify MCH professionals’
strengths and learning needs, match MCH professionals’ learning
needs to appropriate trainings, and receive a personalized learning
plan. The online self-assessment can provide a personalized learning
plan for individual staff, and can track increases in knowledge and
skills longitudinally. State Title V agencies can use the
self-assessment tool for individual staff members, or as a group
within Title V to identify professional development needs and
interests, and identify free learning opportunities to advance
knowledge and skill. Title V agencies can also request a
state-specific snapshot of workforce demographics and
knowledge/skills across the MCH Leadership Competencies, based on
results of the self-assessment.
The
self-assessment tool and information on state snapshots can be found
the MCH Navigator website (described below).
MCH
Navigator
https://www.mchnavigator.org/
The
MCH Navigator is a centralized portal for pursuing continuous
learning in maternal and child health (MCH) and is designed to help
emerging and established MCH professionals and students map
professional growth pathways. The MCH Navigator includes a range of
learning opportunities tailored to MCH professionals and can be
accessed through both self-directed learning or semi-structured
learning. State Title V programs can use the MCH Navigator to assist
with orientation and onboarding of new staff, to develop individual
learning plans, and to conduct group learning or training activities
on topics related to MCH core competencies, knowledge and skill
areas. State Title V staff can use the MCH Navigator to and to
complete the self-assessment tool noted above.
The
National Maternal and Child Health Workforce Development Center
https://mchwdc.unc.edu/
The
National Maternal and Child Health Workforce Development Center (the
Center) helps state and territorial Title V leaders and their
partners tackle complex challenges through training, collaborative
learning, coaching, and consultation. Through the Center’s
customized workforce development offerings, State Title V leaders and
staff identify a health transformation challenge and develop skills
and knowledge to apply in real-time to their state-specific
challenge. State Title V programs can also access Center-developed
self-paced trainings via the MCH Navigator (described above). The
Center’s website also includes resources for Title V agencies
to identify the skills and knowledge needed to support work aligned
with each of the 15 National Performance Measures. State Title V
programs can also access a list of “Foundational Skills”
needed to support all Title V National Performance Measures.
APPENDIX K: GLOSSARY
A comprehensive glossary of terms relevant to maternal and child health (MCH) practice, including services for children with special health care needs (CSHCN), is available on the MCH Navigator site. To access the Glossary, click on: (https://www.mchnavigator.org/documents/Glossary_of_MCH_Terms_and_Acronyms_2012-11-17.pdf). This project is administered by Georgetown University through funding provided by the Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB.) The MCH Navigator is a learning portal for MCH professionals, students, and others working to improve the health and well-being of women, children, adolescents, and families.
Definitions included in this Glossary are intended to supplement the broader set of terms that are included in the MCH Navigator Glossary. The following list of terms and their definitions have specific relevance to the State Title V MCH Block Grants.
Comprised of the following two main sections, the Glossary is intended to assist State Title V programs in completing the yearly Title V MCH Block Grant Application/Annual Report.
Supplemental Program Information (which includes multiple sub-sections); and
Definitions of Program-Relevant MCH Terms.
A Table of Contents is included on the following page to provide an overview for users on the organizational structure of the Glossary and to enable a reader to go directly to a specific section.
Table of Contents
Supplemental Program Information 106
Forms 2-3 – Budget and Expenditures 106
Form 5 – Title V Program Participation and Reach 107
Form 6—Medicaid Eligible Deliveries and Infants Served by Title V 111
Form 10 – Performance Measurement 112
Title V Program Administration 113
Collaborative Learning, Innovation and Quality Improvement 114
Children with Special Health Care Needs 117
Emergency Planning and Preparedness 118
Definitions of Title V Program-Relevant MCH Terms 119
Supplemental Program Information
Reporting Forms
Forms 2-3 – Budget and Expenditures
Administrative Title V Funds - The amount of funds the state uses for the management of the Title V allocation. This amount is limited by statute to 10 percent of the Federal Title V allotment.
Capacity – Program capacity includes delivery systems, workforce, policies, and support systems (e.g., training, research, technical assistance, and information systems) and other infrastructure needed to maintain service delivery and policy making activities. Program capacity results measure the strength of the human and material resources necessary to meet public health obligations. As program capacity sets the stage for other activities, program capacity results are closely related to the results for process, health outcome, and risk factors. Program capacity results should answer the question, “What does the state need to achieve the results we want?”
Budget Period – Period of time for which funds are available for use by the state. For the MCH Block Grant, the budget period is 24 months, beginning on October 1 of the federal fiscal year in which the funds are awarded and ending on September 30 of the following federal fiscal year.
Children – A child from age one (1) through 21 years.
Federal Allocation – The funding provided to the states under the Federal Title V Block Grant in any given fiscal year; applies specifically to the Application Face Sheet (SF-424) and Form 2.
Federal Fiscal Year: The federal government’s fiscal year begins on October 1 and ends on September 30 of the following year.
Infants – Children in their first year of life (<365 days).
Local – Funds derived from local health jurisdictions within the state, which are used for MCH program activities and reported on the Application Face Sheet (SF 424) and Form 2.
Maintenance of Effort – State will maintain the level of funds being provided solely by such state for maternal and child health programs at a level at least equal to the level provided in fiscal year 1989.
Others (Class of Individuals) – Women and men, over age 21.
Other Federal Funds – Federal funds other than the Title V Block Grant that are under the control of the person responsible for administration of the Title V program and reported on the Application Face Sheet (SF 424) and Form 2. These funds may include, but are not limited to: WIC, EMSC, Healthy Start, SPRANS, HIV/AIDs monies, CISS funds, MCH targeted funds from CDC, MCH Education funds and Medicaid Federal Medical Assistance Percentage (FMAP).
Pregnant Woman – A female from the time that she conceives to 60 days after birth, delivery, or expulsion of fetus.
Program Income – Funds collected by State MCH agencies from sources generated by the State’s MCH program to include insurance payments, Medicaid reimbursements, HMO payments, etc., as reported on the Application Face Sheet [SF 424] and Form 2.
State Funds – Non-federal funds derived from the state, as reported on the Application Face Sheet [SF 424] and Form 2, which are used for program activities and to meet the legislatively mandated match requirements (including overmatch, if applicable) for expenditure of the federal Title V MCH Block Grant allocation and the 1989 Maintenance of Effort, in any given year.
Total MCH Funding – All of the MCH funds administered by a State MCH program. Included in this sum total are: 1) the Federal Title V Block grant allocation; 2) the State’s dedicated funds towards meeting the required match for the federal Title V allocation (match and overmatch); 3) the Local funds, which are the total amount of MCH dedicated funds from local government within the state); 4) Other Federal funds (monies other than the Title V Block Grant that are under the control of the person responsible for administration of the Title V program), and 5) Program Income (funds collected by State MCH agencies from insurance payments, Medicaid, HMO’s, private grants, etc.)
Form 5 – Title V Program Participation and Reach
MCH Working Framework: MCH Pyramid of Services0
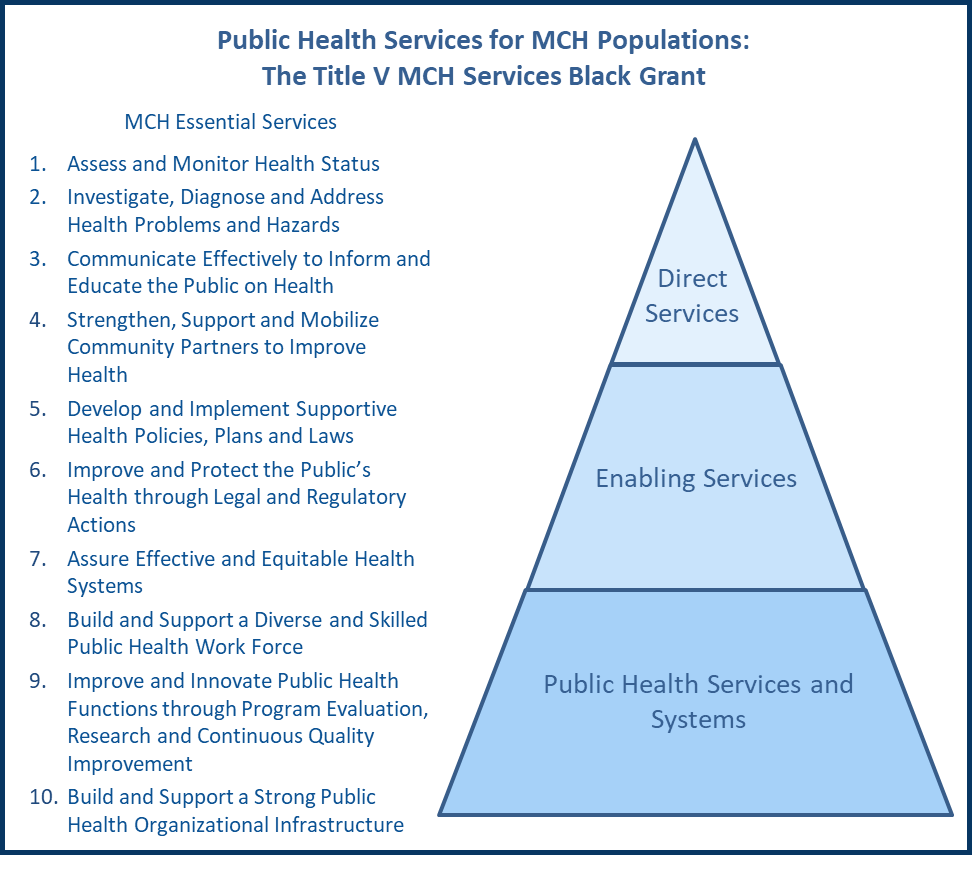
As depicted on the MCH Pyramid, the working framework for the MCH Block Grant aligns with the 10 MCH Essential Services and consists of three levels. Definitions are provided below for each level of service. In developing systems of care, states should assure that they are family-centered, community-based and culturally competent.
Direct Services – Direct services are preventive, primary, or specialty clinical services to pregnant women, infants and children, including children with special health care needs, where MCH Services Block Grant funds are used to reimburse or fund providers for these services through a formal process similar to paying a medical billing claim or managed care contracts. State reporting on direct services should not include the costs of clinical services which are delivered with Title V dollars but reimbursed by Medicaid, CHIP or other public or private payers. Examples include, but are not limited to, preventive, primary or specialty care visits, emergency department visits, inpatient services, outpatient and inpatient mental and behavioral health services, prescription drugs, occupational and physical therapy, speech therapy, durable medical equipment and medical supplies, medical foods, dental care, and vision care.
Enabling Services – Enabling services are non-clinical services (i.e., not included as direct or public health services) that enable individuals to access health care and improve health outcomes where MCH Services Block Grant funds are used to finance these services. Enabling services include, but are not limited to: case management, care coordination, referrals, translation/interpretation, transportation, eligibility assistance, health education for individuals or families, environmental health risk reduction, health literacy, and outreach. State reporting on enabling services should not include the costs for enabling services that are reimbursed by Medicaid, CHIP, or other public and private payers. This category may include salary and operational support to a clinic that enable individuals to access health care or improve health outcomes. Examples include the salary of a public health nurse who provides prenatal care in a local clinic or compensation provided to a specialist pediatrician who provides services for children with special health care needs. In both cases the direct services might still be billed to Medicaid or other insurance, but providing for the availability of the provider enables individuals to access the services.
Public Health Services and Systems – Public health services and systems are activities and infrastructure to carry out the core public health functions of assessment, assurance, and policy development, and the 10 essential public health services. Examples include the development of standards and guidelines, needs assessment, program planning, implementation, and evaluation, policy development, quality assurance and improvement, workforce development, and population-based disease prevention and health promotion campaigns for services such as newborn screening, immunization, injury prevention, safe-sleep education and anti-smoking. State reporting on public health services and systems should not include costs for direct clinical preventive services, such as immunization, newborn screening tests, or smoking cessation.
Number of Individuals and Percentage of Populations Served by Title V (Form 5)
Form 5a, Count of Individuals Served by Title V, enables the state to track and report on the number of who received an individually-delivered service funded in part or in full by the Title V program within the top two levels of the MCH Pyramid (direct and enabling services). This includes individuals receiving services funded by total Federal and State dollars reported on line 8 of Form 2, and should align with the combined totals on Form 3a and 3b for direct and enabling services. Data sources are typically reimbursement or individual client records. Pregnant women may also receive non-pregnancy related services and be counted in other participant categories (i.e. children ages one (1) through 21 and others). All remaining categories are mutually exclusive with CSHCN reported as a subset of all infants and children ages zero (0) through 21. Within each reporting category, the count of individuals served should be unduplicated to the fullest extent possible. Examples of direct and enabling services by participant category that Title V may fund in part or in full are provided below.
Pregnant women (through 60 days postpartum) – payment for prenatal, delivery, or postpartum care, case management, insurance eligibility assistance, hotline calls.
Infants (less than age one) – payment for well child visits, immunization, case management.
Children ages one (1) through 21– payment for well child visits, immunization, dental sealants, school-based health center services.
Children with special health care needs (ages 0 through 21) – specialty care services, care coordination.
Others (women and men over 21) – payment for well-woman visits, education or family-centered care provided to parents/guardians of children.
Form 5b, Total Percentage of Populations Served by Title V, enables the state to track and report on the total percentage who received a Title V-supported service within all levels of the MCH Pyramid (direct services, enabling services, and public health services and systems). The purpose of this form is to better capture the breadth of the State’s Title V program and its reach in serving the MCH population. Included in this reporting are all individuals and populations served by the total Federal and State dollars, as reported on line 8 of Form 2, and the combined totals on Form 3a and 3b for all service levels. Non-Title V programs that provide direct and enabling services (e.g., WIC and Home Visiting) may be included if Title V funds or staff time are used to promote or enhance services. (Individual services that are Title V-funded may also be counted in Form 5a.) To avoid duplication, numerators for the percentage estimate should focus on the programs and services that have the largest reach for a given population, which generally involves the public health services and systems level of the MCH Pyramid. Approximate denominators for each population group will be provided to facilitate percentage estimation. Within public health services and systems, only those reached by activities directly connected to promoting the access or quality of specific population-based services and systems should be counted. Examples of these public health services and systems activities, as well as direct/enabling service partnerships, are provided below by participant category.
Pregnant women (through 60 days postpartum)
Develop and/or maintain a system of risk-appropriate perinatal care designations and transfer protocols (count 100%).
Fund local health departments to engage provider groups and promote screening for perinatal depression, smoking or substance use (count number or percent of births in funded counties).
Partner with Medicaid or other health plans to implement a policy/procedural change to reduce low-risk cesarean delivery or promote smoking cessation (count number or % served by Medicaid or other health plans).
Outreach to hospitals to institute a safe sleep or baby friendly policy, distribute educational materials, or participate in a QI collaborative (count number or % of births in participating hospitals).
Partner with WIC or home visiting programs to provide staff training or otherwise promote education, screening, or referrals on smoking cessation or preventive dental services (count number or % of pregnant/postpartum women served).
Infants (less than age one)
Administer, develop guidelines/standards/policies, or otherwise assure the newborn screening program (count 100%).
Develop and/or maintain a system of risk-appropriate perinatal care designations and transfer protocols (count 100%).
Outreach to hospitals to institute a safe sleep or baby friendly policy, distribute educational materials, or participate in a QI collaborative (count number or % of infants served).
Partner with WIC or home visiting programs to provide staff training or otherwise promote education/counseling on safe sleep practices (count number or % of pregnant/postpartum women served).
Implement a statewide campaign to promote safe sleep practices (count number of Web hits).
Children ages one (1) through 21
Develop and maintain a statewide registry for developmental screening and follow-up (count number of children age one (1) through 5).
Develop or promote school-based injury prevention, oral health, or physical activity programs (count number of children in participating schools).
Partner with Medicaid, health plans, pediatric practices, or schools to implement a policy/procedural change, QI collaborative, or other campaign to promote the adolescent well visit (count number of adolescents enrolled or served by plan/practice/school).
Fund local health departments to promote and advance the medical home model among all pediatric providers (count number of children in local counties).
Children with special health care needs ages 0 through 21 (Examples from Appendix I)
Population-based approaches for the broader child population with CSHCN as a subset:
See examples above and use the same percentage estimated for all children, assuming that CSHCN are served at the same rate since they are not excluded. CSHCN specific data can be used, if available, but it may underestimate reach if the definition does not match the MCHB definition of CSHCN used as a denominator.
Train non-licensed health professionals, including CSHCN parent consultants, to address the social determinants of health (count estimated annual case-loads of those trained or % of professionals trained as a proxy for % of children potentially reached).
Population-based approaches for CSHCN specifically:
Partner with state managed care organization to assess CSHCN quality of life measures for QI efforts (count number or % of CSHCN served by state managed care organization)
Implement a pediatric sub-specialty telemedicine program to ensure access for rural CSHCN (count rural or all CSHCN if system is designed for overall access)
Population-based approaches for a subset of CSHCN:
Partner with Medicaid to implement a Latino-focused care coordination program (count Latino CSHCN covered by Medicaid)
Implement a QI project to promote transition to adult health care for medically complex CSHCN (count medically complex youth with special health care needs)
Others (women and men over age 21)
Implement a statewide campaign to promote the well-woman visit (count number of web hits)
Partner with WIC or Home Visiting to improve screening/counseling for smoking cessation (count number of women with a child age one (1) or more to avoid duplication with pregnant women)
Partner to promote family engagement services (count number of parents over 21 served)
Form 6—Deliveries and Infants Served by Title V and Eligible for Medicaid
Title V of the Social Security Act – The authorizing legislation for the Maternal and Child Health Services Block Grant to States Program.
Title V Reporting Form 6, Deliveries to Pregnant Women Served by Title V – Unduplicated number of deliveries to pregnant women who were provided prenatal, delivery, or post-partum services through the Title V program during the reporting period.
Title V Reporting Form 6, Infants Served by Title V – The unduplicated count of infants provided services by the State’s Title V program during the reporting period.
Title XIX of the Social Security Act – The authorizing legislation for the Medicaid program.
Title XIX Reporting on Form 6, Pregnant Women Eligible for Title XIX – The number of pregnant women who delivered during the reporting period and were eligible for the State’s Title XIX (Medicaid) program.
Title XIX Reporting on Form 6, Infants Eligible for Title XIX – The number of infants eligible for the State’s Title XIX (Medicaid) program.
Title XXI of the Social Security Act – Children’s Health Insurance Program (CHIP) financed via the Centers for Medicare and Medicaid Services (CMS). The purpose of this title is to provide funds to states to enable them to initiate and expand the provision of child health assistance to uninsured, low-income children in an effective and efficient manner that is coordinated with other sources of health benefits coverage for children. (Sec. 2101. [42 U.S.C. 1397aa])
Form 10 – Performance Measurement
Evidence-based or –Informed Strategy Measure (ESM) –Developed by the state, ESMs assess the outputs of State Title V strategies and activities contained in the State Action Plan. The development of ESMs is guided through an examination of evidenced-based or evidence-informed strategies, and determining what components are meaningful, measurable, and achievable. The main criteria for ESMs are in being meaningfully related to the selected NPM through scientific evidence or theory and being measurable by the state with improvement achievable in multiple years of the five-year reporting cycle.
Evidence-based or –Informed Strategy Measure (ESM) Objectives – The objectives for activities and interventions that drive the achievement of higher-level objectives by the State Title V program.
Objectives – The yardsticks by which an agency can measure its efforts to accomplish a goal. (See also Performance Objectives)
Outcome Measure – The ultimate focus and desired result of any set of public health program activities and interventions is an improved health and well-being outcome. Health and well-being outcomes are usually longer term and tied to the ultimate program goal. Morbidity and mortality statistics are indicators of achievement of health outcomes. For the Title V performance framework, other outcomes reflect commonly accepted indicators of a highly functioning system of care for children with special health care needs and their families, positive outcomes, outcomes which are legislatively mandated or are a legislative focus, and outcomes where the prevalence is increased.
Performance Indicator – The statistical or quantitative value that expresses the result of a performance objective.
Performance Measure – An intermediate outcome on the path toward a longer term outcome measure of health and well-being that is used to more directly assess the impact of a program. Positive health behaviors and access to quality health care are common intermediate outcomes that may lead to health, reduced morbidity and mortality, or highly functioning systems of care. For example, to reduce infant mortality, State Title V programs may work to promote safe sleep practices or access to quality well-woman care. The performance measure is phrased as a quantitative indicator, such as a rate or percentage. For example, “Percentage of infants placed to sleep on their backs.”
Performance Measurement – The collection of data on, recording of, or tabulation of results or achievements, usually for comparison to a benchmark.
Performance Objectives – A statement of intention with which actual achievement and results can be measured and compared. Performance objective statements clearly describe what is to be achieved, when it is to be achieved, the extent of the achievement, and the target populations. For example: “Increase the percentage of infants placed to sleep on their backs in State X by 10% over the next 5 years.”
Risk Factors – Public health activities and programs that focus on reduction of scientifically established direct causes of, and contributors to, morbidity and mortality (i.e., risk factors) are essential steps toward achieving desired health outcomes. Changes in behavior or physiological conditions are the indicators of achievement of risk factor results. Results focused on risk factors tend to be intermediate term. Risk factor results should answer the question, “Why should the state address this risk factor (i.e., what health outcome will this result support)?”
Risk Factor Objectives – Objectives that describe an improvement in risk factors (usually behavioral or physiological) that are associated with morbidity and mortality.
Targets – An aspired outcome that is explicitly stated, e.g. “Attain 90% of timeliness in reporting” or ”Achieve 100% completeness of reporting”, etc. In this Guidance, “Targets” is often used interchangeably with “Objectives.”
Title V Program Administration
Data Systems Development – Development of data management systems (electronic or other) or linking of existing databases to support states’ ability to collect, tabulate, analyze, and report data accurately.
Government Performance and Results Act (GPRA) – Federal legislation enacted in 1993 that requires Federal agencies to develop strategic plans, prepare annual plans setting performance goals, and report annually on actual performance.
Jurisdictions – The following nine jurisdictions receive Title V Maternal and Child Health Block Grant Program funding: the District of Columbia, the Republic of the Marshall Islands, the Federated States of Micronesia, the Republic of Palau and the U.S. territories of the Commonwealth of Puerto Rico, the Virgin Islands, Guam, American Samoa, and the Commonwealth of the Northern Mariana Islands.
Life Course Theory (LCT) – A conceptual framework that helps explain health and disease patterns, particularly health disparities, across populations and over time. Instead of focusing on differences in health patterns based on one disease or condition at a time, LCT points to broad social, economic and environmental factors as underlying causes of persistent inequalities in health for a wide range of diseases and conditions across population groups. LCT is population focused, and firmly rooted in social determinants and social equity models. Though not often explicitly stated, LCT is also community (or “place”) focused, since social, economic and environmental patterns are closely linked to community and neighborhood settings.0
Needs Assessment – A process to understand the strengths and needs of the health service system within a community or population. For maternal and child health purposes, needs assessment efforts consider the following components: 1) health status, 2) health service
utilization, 3) health systems capacity, and 4) population/ community characteristics and contextual characteristics.
Objectives – A statement of intention with which actual achievement and results can be measured and compared. SMART objectives are Specific, Measurable, Achievable, Relevant and Time-phased. See also Objectives and Performance Objectives within the Performance Measurement Section.
Priority Needs – Title V legislation direct states to conduct a statewide, comprehensive MCH Needs Assessment every five years to identify the need for preventive and primary care services for pregnant women, mothers, infants, children and children with special health care needs. From this assessment, states select seven to ten priorities for focused programmatic efforts over the five-year reporting cycle.
State – Terminology used in this Guidance to reference the 50 states and the nine jurisdictions. (See also “Jurisdictions”)
Strategies – General approaches taken to achieve objectives: activities are specific actions to implement the strategies. For example, a strategy may be to improve provider training with activities that could include developing a training module, delivering or promoting the training, and monitoring utilization and/or knowledge improvement. Program activities for implementing the identified program strategies are discussed and updated annually as part of the State Action Plan narrative.
Technical Assistance (TA) – The process of providing advice, assistance, and training by an expert with specific technical/content knowledge to address an identified need. Technical Assistance relationships are program-focused, and may use an interactive, on-site/hands-on approach as well as telephone or email assistance. Technical Assistance delivery is short in duration, customized to meet the needs of the client, and offers prescriptive solutions to a specific issue.
Collaborative Learning, Innovation and Quality Improvement
Aim Statement – A written measureable description of desired outcomes used in a quality improvement initiative. A strong AIM statement outlines what is to be accomplished, quantifies the changes that are to be achieved and sets a date by which the goals will be reached.
Blueprint for Change – A tool to help define action steps for a team’s strategic priorities.
CoIIN versus COIN – The Collaborative Improvement and Innovation Network (CoIIN) initiative extends the Collaboration Innovation Network (COIN) model to include the concept of improvement in recognition of the need to strengthen existing investments in maternal and infant health as well as to develop innovative, new approaches.
Collaborative Innovation Network (COIN) – A cyberteam of self-motivated people with a collective vision, enabled by the Web to collaborate in achieving a common goal by sharing ideas, information and work.0
Collaborative Learning – Projects using this model enable learners of different abilities and interests to work jointly in small groups to complete a project or solve a problem.
Collective Impact – A concept that provides a framework for bringing diverse people and organizations together in a structured way to achieve social change.0
Driver Diagram – A logic chart that organizes the different aspects of an improvement project so key interventions and relationships between these interventions may be clearly understood by all involved.
Infant Mortality CoIIN Framework – A framework that presents a theory of the relationships between (1) key domains of influence (e.g., engaged leadership or innovation), (2) the periods of engagement, and (3) the strategies priorities that will be employed to reduce infant mortality rates in the U.S.
Learning Collaborative – A group of individuals or organizations that come together for a defined period of time to work together to improve process relevant to a specific topic. Members of a learning collaborative generally agree upon a shared set of data to measure and meet regularly to learn from each other and project experts.
Learning Sessions – Members of learning collaboratives generally agree to a regular schedule of multi-day meetings throughout the collaborative. These meetings may be in person or virtual. The learning sessions allow Collaborative faculty and partners to share latest research or important information on the topic of the collaborative, and they allow participants to share their work and to learn from each other.
Perinatal Periods of Risk (PPOR) – Both a community approach and an analytic framework for investigating and addressing high infant mortality rates in urban settings. The overall intent of the PPOR approach is to develop a simple method that can be used by communities to mobilize and prioritize prevention efforts. PPOR brings community stakeholders together to build consensus, support and partnership around infant mortality rates.0
Primary Drivers – Found in the CoIIN framework and driver diagrams, drivers are system components, factors or broad improvement areas that contribute directly to achieving the stated outcome. For example, if the outcome is reducing infant mortality, a strategic priority/primary driver might be to improve access to and quality of prenatal care for women. (See Strategic Priorities.)
Potential Action/Change Concept – Actionable steps for change targeted at improving specific processes, often originating from brainstorming sessions with the team and evidence-based best practices.
Quality Improvement in Public Health – The use of a deliberate and defined improvement process, which is focused on activities that are responsive to community needs and improving population health. This effort is continuous and ongoing to achieve measureable improvements in the efficiency, effectiveness, performance, accountability, outcomes and other indicators of quality in services or processes, which achieve equity and improve the health of the community.
Strategic Priorities – Found in the CoIIN framework and driver diagrams, these priorities are system components, factors or broad improvement areas that contribute directly to achieving the stated outcome. For example, if the outcome is reducing infant mortality, a strategic priority/primary driver might be to improve access to and quality of prenatal care for women.
Cultural Competence – A set of values, behaviors, attitudes, and practices within a system, organization, program or among individuals and which enables them to work effectively cross culturally. Further, cultural competence refers to the ability to honor and respect the beliefs, language, inter-personal styles and behaviors of individuals and families receiving services, as well as staff who are providing such services.
Culturally Sensitive – The recognition and understanding that different cultures may have different concepts and practices with regard to health care; the respect of those differences and the development of approaches to health care with those differences in mind.
Family Partnership – For purposes of the MCH Block Grant, family partnership is defined as patients, families, their representatives, and health professionals working in active partnership at various levels across the health care system—direct care, organizational design and governance, and policy making—to improve health and health care. 0 This partnership is accomplished through the intentional practice of working with families for the ultimate goal of positive outcomes in all areas through the life course. Additional references include, but are not limited to, several comprehensive reports written by the Association of Maternal and Child Health Programs (AMCHP) that describe family engagement efforts in State Title V programs. These references are available at: http://www.amchp.org/programsandtopics/family-engagement/Pages/default.aspx.
Patient- and Family-Centered Care – “An approach to the planning, delivery, and evaluation of health care that is grounded in a mutually beneficial partnership among patients, families, and providers that recognizes the importance of the family in the patient’s life.”0 “This approach recognizes that the perspectives and information provided by families, children, and young adults are essential components of high-quality clinical decision-making, and that patients and family are integral partners with the health care team.”0
Children with Special Health Care Needs
Care Coordination Services – Services that promote the effective and efficient organization and utilization of resources to assure access to necessary comprehensive services for children with special health care needs and their families. [Section 501(b)(3)] Pediatric care coordination is “patient and family centered, assessment driven, team based.0 Care coordination services facilitate linkage of children and their families with appropriate services and resources that meet their health and social needs to achieve optimal health. This care is to be distinguished from case management which primarily focuses on the children’s medical issues.0
Case Management Services – Services that assure access to quality prenatal, delivery and postpartum care for pregnant women; and services that assure access to quality preventive and primary care services for infants up to age one (1). [Section 501(b)(4)]
Children With Special Health Care Needs (CSHCN) – Children with special health care needs are those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.0 For Form 5 reporting, infants with special health care needs (0-12 months) and CSHCN ages one (1) through 21 are captured separately as a subset under children. The reported totals for all infants and children should include infants and children who have special health care needs.
Systems of Services for Children with Special Health Care Needs – A system of services for children with special health care needs is a “family-centered coordinated network of community-based services designed to promote the healthy development and well-being of children and their families”.0 Additionally, a “well-functioning system of services will coordinate and integrate the full range of needed child and family services, including health care, education, and social services, with the goal of optimizing outcomes for the children and families it serves.”0
Key frameworks describing the system of services for CSHCN:
Six Core Outcomes for CSHCN0,0
Family Professional Partnership
Medical Home
Adequate Health Insurance
Early and Continuous Screening and Surveillance
Easy to Use Services and Supports
Transition to Adult Health Care
National Standards for Systems of Care for Children and Youth with Special Health Care Needs
The National Systems Standards describe the process and provide a framework necessary to build an effective system of services for CSHCN. The standards are divided into ten core domains, and they are based on the six core outcomes listed above for CSHCN. Additional information is available at: http://www.amchp.org/AboutTitleV/Resources/Documents/Standards%20Charts%20FINAL.pdf.
Emergency Planning and Preparedness0
Emergency – Any incident, whether natural, technological, or human-caused, that necessitates responsive action to protect life or property.
Emergency Operations Center (EOC) – The physical location where the coordination of information and resources to support incident management (on-scene operations) activities normally takes place.
Emergency Operations Plan (EOP) – A plan for responding to a variety of potential hazards.
Incident Management – The broad spectrum of activities and organizations providing operations, coordination, and support applied at all levels of government, using both governmental and nongovernmental resources to plan for, respond to, and recover from an incident, regardless of cause, size, or complexity.
Mission Area – One of five areas (Prevention, Protection, Mitigation, Response, and Recovery) designated in the National Preparedness Goal to group core capabilities.
Mitigation – The capabilities necessary to reduce the loss of life and property from natural and/or manmade disasters by lessening the impacts of disasters.
Prevention – The capabilities necessary to avoid, prevent, or stop a threatened or actual act of terrorism. In national preparedness guidance, the term “prevention” refers to preventing imminent threats.
Protection – The capabilities necessary to secure the homeland against acts of terrorism and manmade or natural disasters.
Recovery – The capabilities necessary to assist communities affected by an incident to recover effectively.
Response – The capabilities necessary to save lives, protect property and the environment, and meet basic human needs after an incident has occurred.
Definitions of Title V Program-Relevant MCH Terms
Acquired Brain Injury – Injury to the brain that is not hereditary, congenital, degenerative, or induced by birth trauma. Traumatic brain injury is a type of acquired brain injury.
Bullying – Unwanted, aggressive behavior among school aged children that involves a real or perceived power imbalance. The behavior is repeated, or has the potential to be repeated, over time. Additional guidance on bullying surveillance is available at: http://www.cdc.gov/violenceprevention/pdf/bullying-definitions-final-a.pdf.
Clinical Genetics – Clinical and laboratory services for individuals and families with, or at risk for, health problems with a heritable component. The application of the principles of genetics and genomics to predict, diagnose, and treat disease and improve health.
Community – A group of individuals living as a smaller social unit within the confines of a larger one due to common geographic boundaries, a common work environment, common interests and other uniting factors.
Community-based Care – Services provided within the context of a defined community.
Community-based Service System – An infrastructure that operates across service sectors that facilitates the integration of services in several dimensions, which includes organization, delivery, and financing.0
Early Neonatal Period – Period covered by the first week after birth or an age of less than seven days.
Genetic Counseling: The process of helping people to understand and adapt to the medical, psychological, and familial implications of genetic contributions to disease. This process integrates: interpretation of family and medical history to assess the chance of disease occurrence or recurrence; education about inheritance, testing, management, prevention,
resources and research; counseling to promote informed choices; and adaptation to the risk or condition.
Health Care System – The entirety of the agencies, services, and providers involved or potentially involved in the health care of community members and the interactions among those agencies, services and providers.
Human Genetics: The science of genes, heredity and variation in human organisms.
Health Care Transition – The process of moving from a child to an adult model of health care. The goal of health care transition (HCT) is to optimize health and assist youth in reaching their full potential, which requires an active process over time that addresses many aspects of a youth’s life, including medical, psychosocial, educational, and vocational needs. This process also ensures continuity of developmental and age appropriate health care services. Successful transition involves the engagement and participation of the pediatric and adult medical home team, the family and other care givers, and the individual youth collaborating in a positive and mutually respectful relationship.0 For more information see http://www.gottransition.org/
Low Income – An individual or family with an income that is determined to be below the income official federal poverty line, as defined by the Office of Management and Budget and revised annually in accordance with 42 U.S.C. 9902(2). [Section 501(b)(2)]
Medical Home – An approach to providing comprehensive, high quality health care that is accessible, family-centered, continuous, comprehensive, coordinated, compassionate and culturally effective.0 Care occurs in an environment of trust and mutual responsibility between the family, patient, and primary care provider. The principle of family-centered care defines the care to be received in a medical home while a team-based approach is central to delivering care in the medical home. Within the medical home, care coordination addresses interrelated medical, dental, mental and behavioral, social, educational, and financial needs to achieve optimal health and wellness outcomes. Additional information is available at: https://medicalhomeinfo.aap.org/Pages/default.aspx.
Morbidity – A general term for any health condition that encompasses diseases, injuries, and impairments in a population or group.
Mortality – A general term for the incidence of deaths in a population or group. The number of deaths may be reported by age, sex, race/ethnicity, geographic area, and cause of death.
Mortality Rate – The number of deaths occurring in a particular population during a specific time period, as calculated by the number of deaths in that group (numerator) divided by the total population (denominator) and expressed as per 1,000 live births (infant mortality rate only) or per 100,000 population, generally at mid-year.
National Improvement Partnership Network (NIPN) – A network of states who have an Improvement Partnership (IP), which is a durable collaborative of public and private partners that use the science of quality improvement and a systems approach to improve health care infrastructure and practice. Established in 2009, NIPN is led by the Vermont Child Health Improvement Program (VCHIP).
National Survey of Children’s Health (NSCH) – Sponsored by the Maternal and Child Health Bureau of the Health Resources and Services Administration, the NSCH examines the physical and emotional health status and health service needs and utilization patterns of children ages 0-17 years of age. Special emphasis is placed on factors that may relate to well-being of children, including medical homes, family interactions, parental health, school and after-school experiences, and safe neighborhoods. The NSCH was fielded three times as a telephone-based survey, in 2003, 2007 and 2011-2012, yielding both state- and nationally-representative data. In 2016, the NSCH underwent a significant redesign, becoming an annual address-based mailed survey with a web-based response option that merged content from the previous NSCH and National Survey of Children with Special Health Care Needs (NS-CSHCN). https://mchb.hrsa.gov/data/national-surveys
National Survey of Children with Special Health Care Needs (NS-CSHCN) – This survey was sponsored by the Maternal and Child Health Bureau of the Health Resources and Services Administration. The NS-CSHCN was conducted three times as a telephone-based survey, in 2001, 2005-2006 and 2009-2010, and yielded state- and nationally-representative data on the health care experiences of CSHCN and their families. In 2016, the NS-CSHCN was merged with the NSCH to provide one unified survey administered annually by mail with a web-based response option. Additional information is available at: https://mchb.hrsa.gov/data/national-surveys.
Neonatal Period – period covered by the first month after birth or an age of less than 28 days.
Newborn – A recently born infant, usually less than one month old.
Newborn Screening (NBS) – The process of testing newborn babies for some serious, but treatable, conditions. Four million newborns each year are tested for conditions on the Recommended Uniform Screening Panel (a set of conditions recommended by the Secretary of HHS for NBS) that are not apparent at birth but require early intervention and treatment to mitigate brain and organ damage, severe illness, and life-threatening complications associated with these conditions. NBS can include a heel stick, hearing screen, and pulse oximetry. The conditions that newborn babies are screened for varies by state. When a newborn screening result is out-of-range, further diagnostic testing is required to confirm or specify the results.
Newborn Screening Long-term Follow-up – Comprises the assurance and provision of ongoing quality chronic disease management, condition-specific treatment, and age-appropriate care throughout the lifespan of individuals identified with a condition included in newborn screening.
Newborn Screening Short-term Follow-up – The process of ensuring that all newborns are screened, that an appropriate follow-up caregiver is informed of results, that confirmatory testing has been completed, and that the infant has received a diagnosis and, if necessary, treatment is initiated.
Perinatal – Period pertaining to immediately before and after birth. For example, the definition of perinatal mortality refers to fetal and early neonatal death between 28 weeks or more gestation through the first week of life (less than seven days after birth).
Postneonatal Period – Period of infant age from one month (28 days) up to one year (<365 days).
Prenatal – Occurring or existing before birth, referring to both the care of the woman during pregnancy and the growth and development of the fetus.
Preventive Services – Activities aimed at reducing the incidence of health problems or disease prevalence in the community, or the personal risk factors for such diseases or conditions.
Preventive Oral Health Services – Activities that aim to improve and maintain good oral health and function by reducing the onset and/or development of oral diseases or deformities and the occurrence of oro-facial injuries. Examples of preventive oral health services include, but are not limited to, oral hygiene instructions, fluoride treatment, and Dental Sealants.
Primary Care/Primary Care Services – The provision of comprehensive personal health services that include health maintenance and preventive services, initial assessment of health problems, treatment of uncomplicated and diagnosed chronic health problems, and the overall management of an individual’s or family’s health care services.
Recommended Uniform Screening Panel (RUSP) – The RUSP is a list of disorders that are recommended by the Secretary of the Department of Health and Human Services (HHS) for states to screen as part of their state universal newborn screening (NBS) programs. Disorders on the RUSP are chosen based on evidence that supports the potential net benefit of screening, the ability of states to screen for the disorder, and the availability of effective treatments. It is recommended that every newborn be screened for all disorders on the RUSP. Most states screen for the majority of disorders on the RUSP; newer conditions are still in process of adoption. Some states also screen for additional disorders. Although states ultimately determine what disorders their NBS program will screen for, the RUSP establishes a standardized list of disorders that have been supported by the Advisory Committee on Heritable Disorders in Newborns and Children and the Secretary of HHS.
Safe Infant Sleep Environment – Infant is placed to sleep on its back, in its own crib without blankets or soft items or bed-sharing. Additional information is available at: http://pediatrics.aappublications.org/content/early/2011/10/12/peds.2011-2284
Sudden Unexpected Infant Deaths (SUID) - Deaths in infants less than one year of age that occur suddenly and unexpectedly, and in whom the cause of death is not immediately obvious prior to investigation.
Sudden Infant Death Syndrome (SIDS) – The sudden death of an infant less than one year of age that cannot be explained after a thorough investigation is conducted, including a complete autopsy, examination of the death scene, and review of the clinical history.
Systems Development – Activities involving the creation or enhancement of organizational infrastructures at the community level for the delivery of health services and other needed ancillary services to individuals in the community by improving the service capacity of health care service providers.
Traumatic Brain Injury – An alteration in brain function, or other evidence of brain pathology caused by an external force.
2 Carman K., Dardess, P., Maurer, M., Sofaer, S., Adams, K., Bechtel, C., Sweeney, J. “Patient and Family Engagement: A framework for understanding the elements and developing interventions and policies.” Health Affairs. 2013; 32:223-231.
3 Carman K., Dardess, P., Maurer, M., Sofaer, S., Adams, K., Bechtcl, C., Sweeney, J. Patient and Family Engagement: A framework for understanding the elements and developing interventions and policies. Health Affairs. 2013; 32:223-231
4 Ibid.
5 For purposes of the MCH Block Grant program, children are defined as ages 1 through 21 years. As referenced throughout the Title V MCH Services Block Grant Guidance, the population of CSHCN is inclusive of children and youth.
6 Children and youth with special health care needs have or are at increased risk for chronic physical, developmental, behavioral or emotional conditions and who also require health and related services of a type or amount beyond that required by children generally (McPherson et al., 1998).
7 Section 501(a)(1)(D) of the Title V legislation states that the purpose of the MCH Block Grant is to enable each state to provide and to promote family-centered, community-based, coordinated care (including care coordination services, as defined in subsection (b)(3)) for children with special health care needs (CSHCN) and to facilitate the development of community-based systems of services for such children and their families.
8 Section 501(b)(3) of the Title V legislation includes a definition of “care coordination services.” https://www.ssa.gov/OP_Home/ssact/title05/0501.htm.
9 Kindig D, Stoddart G. What is population health?. Am J Public Health. 2003;93(3):380–383. doi:10.2105/ajph.93.3.380
10 Examples include, but are not limited to, children with medical complexity, CSHCN experiencing disparities by region, race, or condition, and CSHCN in a specific state.
11 Policy may include legislative or organizational policy.
12 Systems involve more than one institution, organization, or agency.
13 Child and Adolescent Health Measurement Initiative. 2017-2018 National Survey of Children’s Health (NSCH) data query. Data Resource Center for Child and Adolescent Health supported by Cooperative Agreement U59MC27866 from the U.S. Department of Health and Human Services, Health Resources and Services Administration’s Maternal and Child Health Bureau (HRSA MCHB). Retrieved 2/5/2020 from www.childhealthdata.org. CAHMI: www.cahmi.org.
14 Maternal and Child Health Leadership Competencies-Version 4.0. Available at https://mchb.hrsa.gov/training/documents/MCH_Leadership_Competencies_v4.pdf
0 10 Essential Public Health Services Futures Initiative Task Force. 10 Essential Public Health Services. September 9, 2020. https://phnci.org/uploads/resource-files/EPHS-English.pdf
0 Gloor, Peter A. “Swarm Creativity.” Competitive Advantage through Collaborative Innovation Networks. (2006)
0 Carman K., Dardess, P., Maurer, M., Sofaer, S., Adams, K., Bechtel, C., Sweeney, J. Patient and Family Engagement: A framework for understanding the elements and developing interventions and policies. Health Affairs. 2013; 32:223-231.
0 Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and Family-Centered Care and the Pediatrician’s Role. Pediatrics. 2012; 129: 394
0 Ibid.
0 Antonelli RC, McAllister J, Popp J. 2009. Developing Care Coordination as a critical component of a high performance pediatric health care system. Washington DC: The Commonwealth Fund
0 Turchi RM, Mann M. Building a medical home for children and youth with special health care needs. In: Hollar D, ed. Handbook of Children with Special Health Care Needs. New York, NY: Springer-Verlag; 2013:399-418.
0 McPherson M., Arango P., Fox H. A new definition of children with special health care needs. Pediatrics. 1998; 102: 137-140.
0 Perrin, J., Romm, D., Bloom, S., Homer, C., Kuhlthau, K., Cooley, C., Duncan, P., Roberts, R., Sloyer, P., Wells, N., Newacheck, P. A family-centered, community-based system of services for children and youth with special health care needs. 2007; 161 (10): 933-936.
0 Ibid.
0 National Agenda for Children with Special Health Care Needs: Achieving the Goals 2000. Washington, D.C.: Health Resources Services Administration; 1999.
0 Strickland, B., van Dyck, P., Kogan, M., Lauver, C., Blumberg, S., Bethell, C., Newacheck, P. Assessing and ensuring a comprehensive system of services for children with special health care needs: a public health approach. 2011; 101 (2): 224-231.
0 Federal Emergency Management Agency (FEMA), June 2020 https://training.fema.gov/emiweb/is/icsresource/assets/glossary%20of%20related%20terms.pdf
0 U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. The National Survey of Children with Special Health Care Needs Chartbook 2009–2010. Rockville, Maryland: U.S. Department of Health and Human Services, 2013.
0 American Academy of Pediatrics. American Academy of Family Physicians and American College of Physicians. Transitions Clinical Report Authoring Group. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. 2011;
0 American Academy of Pediatrics. Organizational principles to guide and define the child health care system and/or improve the health of all children. Pediatrics; 110 (1): 2002
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Edits to detail sheets for Performance Measure Workgroup |
| Author | mlawler |
| File Modified | 0000-00-00 |
| File Created | 2021-01-12 |
© 2025 OMB.report | Privacy Policy