OMB PRA Appendices_NLSOAAP
OMB-PRA Appendices_Redesigned NSOAAP_FINAL_6feb2018.docx
National Survey of Older Americans Act Participants
OMB PRA Appendices_NLSOAAP
OMB: 0985-0023
Application for Data Collection:
National Longitudinal Survey of
Older Americans Act Participants
APPENDICES

February 6, 2018
Submitted by:
U.S. Administration for Community Living Administration on Aging 330 C Street, SW Washington, DC 20201
|
Table
of Contents
Appendices
A Pertinent Legislation
B Baseline and Follow-Up Survey [see separate documents]
C Invitation Letter for Cognitive Testing Participants
D Instructions for AAA Access to the Survey Website & How to Submit Data
E Federal Register Notice Published by ACL/AoA for the Proposed Information Collection
F Westat Assurance of Confidentiality Agreement
G Agency Information Packet
H Reminder Card
I Follow-up Telephone Script
Appendix A
Pertinent Legislation
Pertinent Legislation
Legal Authority: The legal authorities to collect this information are found in the Older Americans Act:
Section 205.(a)(1)(C) of the Older Americans Act (OAA) which gives the Assistant Secretary authority to conduct research and demonstrations; and
Section 206 of the OAA which establishes the authority to measure and evaluate the impact of all programs authorized by the OAA
Additional pertinent legislation:
GPRA Modernization Act of 2010 (GPRAMA)
Section 202(f) of the OAA requires AoA to work collaboratively with State agencies and area agencies on aging (AAAs) to develop performance outcome measures.
Sources:
Older Americans Act: https://www.acl.gov/about-acl/authorizing-statutes/older-americans-act
GPRA Modernization Act of 2010 (GPRAMA):
https://www.gpo.gov/fdsys/pkg/PLAW-111publ352/pdf/PLAW-111publ352.pdf
Appendix B
Baseline and Follow-Up Surveys
Appendix C
Invitation Letter for Cognitive Testing Participants
Sample Letter for Clients Selected for the Cognitive Testing
Tri-County Area Agency on Aging
123 Anywhere St.
Anywhere, XX 12345
<DATE>
Dear Mr./Mrs. ______________________________ ,
We are writing to ask for your help. <<INSERT AAA NAME>> is taking part in a study for the Administration for Community Living (ACL)/Administration on Aging (AoA), part of the U.S. Department of Health and Human Services. ACL/AoA wants to test questions in the National Survey of Older Americans Act Participants to make sure that the question are clear. The National Survey wants to know what people around the country think about the meal programs, transportation, family caregiver, and other services offered by their local AAA.
You have been chosen to be part of the effort to test the questions. An interviewer from Westat, a research firm working for AoA, will call you in the near future to ask you some questions about your experience with <<INSERT AAA NAME & PROVIDER NAME IF KNOWN>>. For some of the questions, the interviewer will ask you to repeat the question in your own words. The interviewer may also ask you to define selected terms in the survey. This will help ACL/AoA make sure that the questions are clear and convey the appropriate meaning.
Your answers will be kept private. Your name won’t be given to anyone else. We will not make a permanent record of your answers to the survey questions. However, we will record your comments about the questions. We will combine your comments with the comments of other respondents. Based on the review of the comments, we will update the questions to make them easier to understand.
I hope you will be part of testing the questions. It’s your choice. Whatever you decide, it won’t affect the services you get now or in the future. If you do not want to take part in this study, please call <<INSERT AAA CONTACT NAME>> at <<INSERT AAA PHONE NUMBER>> by <<INSERT DATE>>.
If you have any questions about this study, please call Westat toll-free at 1-888-204-0046 or the Administration on Aging toll-free at 1-888-204-0271. If you have any questions about the services you get, please call our office at <<INSERT AAA PHONE NUMBER>>.
Thank you for your help and support.
Sincerely,
______________________________,
Executive Director
An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. The OMB control number for this information collection is XXXX-XXXX. Public reporting burden for this information collection is estimated to average 35 minutes per response; response times may range from 20 minutes to 40 minutes. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to the Administration for Community Living/Administration on Aging, Washington, DC 20201 Attn: Dr. Heather Menne, 888-204-0271.
Appendix D
Instructions for AAA Access to the Survey Website &
How to Submit Data
AoA National Longitudinal Survey of Older Americans Act Participants
Instructions for AAA/SUA Access to the Website
To safeguard private, personally identifiable client contact information and to improve communication, we have created a secure website for the AoA National Survey of Older Americans Act Participants. State units on aging and area agencies on aging will be able to submit electronic files containing private client data to Westat via the AoA National Survey web site. Included in the notification packet sent to each SUA and AAA is a separate card with the unique SUA-ID# or AAA-ID # and secure password assigned to your agency that will enable your staff to electronically upload data to the web site.
The web site uses the industry-standard TLS (Transport Layer Security) 1.1/2 encryption for secure data submissions. When files containing client data are uploaded to the website, they are automatically stored in a secure database. The database containing the client data is not accessible via the Internet; it resides on a server inside the Westat firewall. Only Westat Data Collection Program staff members have access to the master survey database.
This document describes how to access the AoA National Survey Web Site: www.aoasurvey.org. You will use this web site to upload your client lists and client contact information and to retrieve sampling results (the list of clients selected to participate in the survey), as well as to download additional instructions and forms.
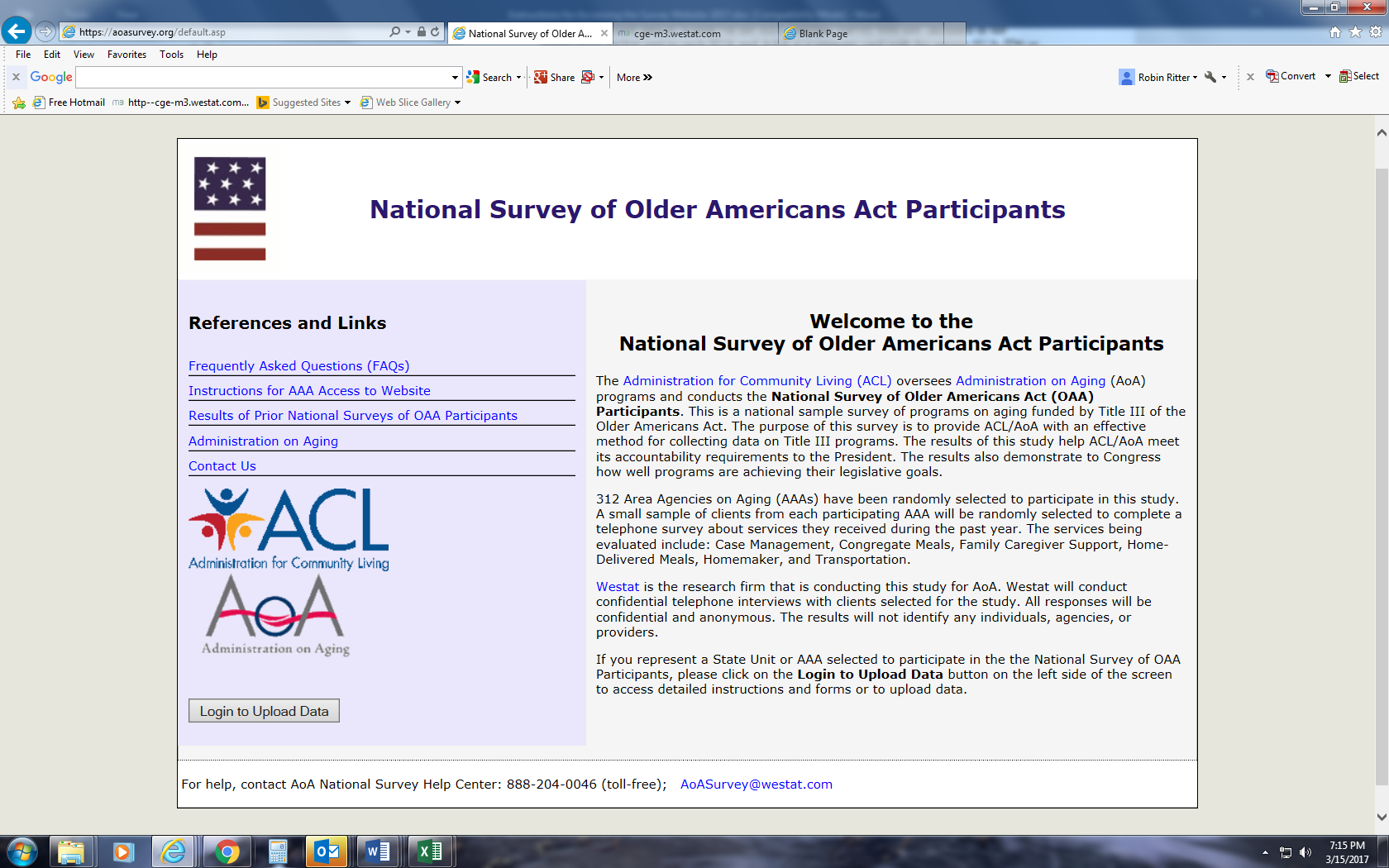
Step 1: Go to www.aoasurvey.org. You will automatically be redirected to https://aoasurvey.org/default.asp.
The Welcome page is available to the general public and can be accessed by any of your clients and their families who wish to know more information about the AoA National Survey.
Step 2: Login to upload data or download instructions and forms.
To login to the secure part of the website, click on Login to Upload Data.

Step 3: At the AAA/SUA Login page, enter your AAA-ID or SUA-ID number and password and click, “Submit.”


Step 4: Upload Client Data; Download Instructions and Forms
This screen is only accessible to SUAs and AAAs that have logged in with their SUA-ID# or AAA-ID# and password. There are two major components to this page:
On the left-side of the web page are copies of instructions and forms that you can download.

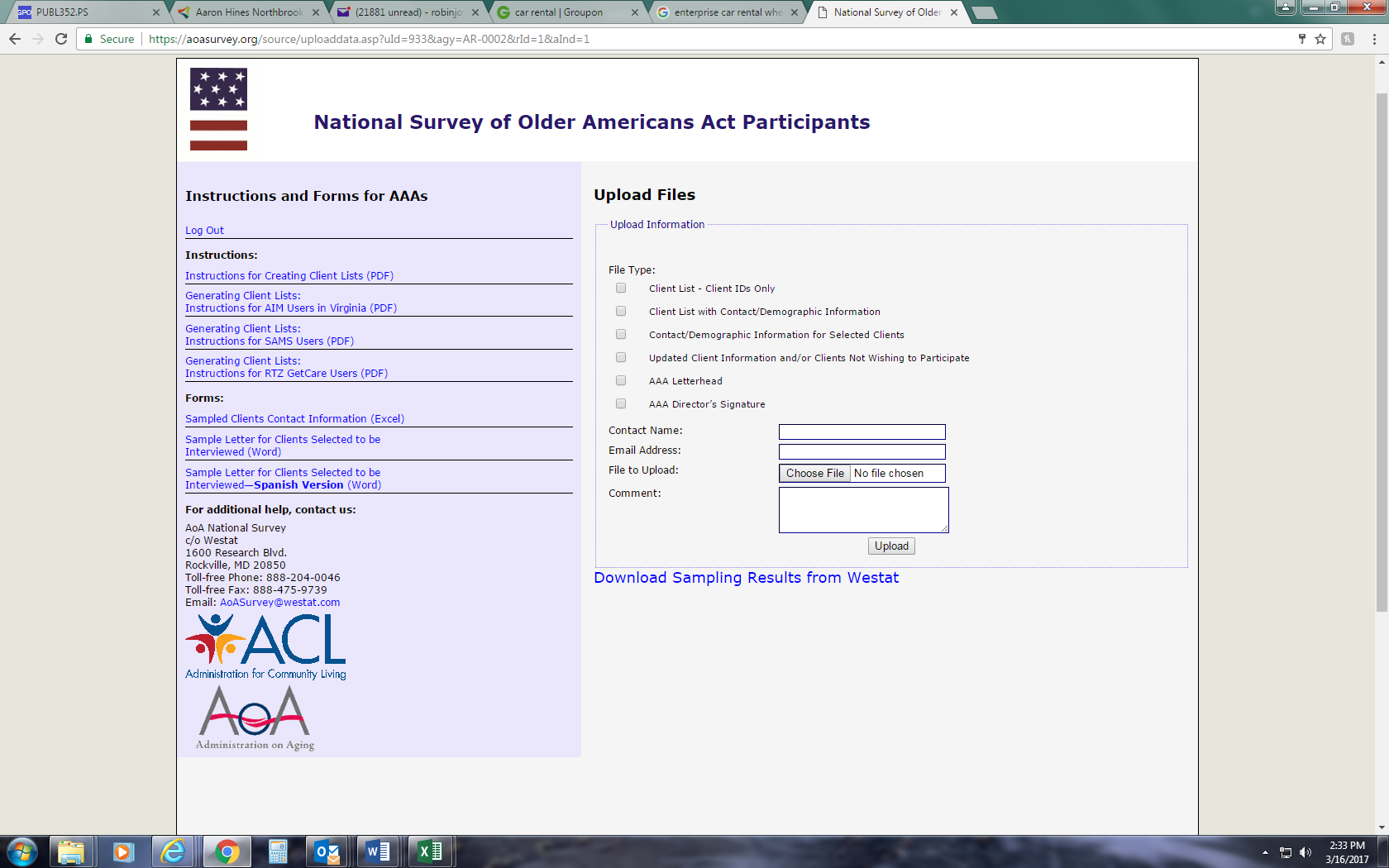
On the right-side of the web page, you can upload your client lists, client contact information, and AAA letterhead and signature.
To upload a file, select File Type and check one of the appropriate six options.
Please fill in the Contact Name and Email Address.
To upload a specific file, click Browse. A window will open which says, Choose File to Upload. Scroll to the folder location to select the file or files you want to upload.

Click on the specific file that you want to upload, and your choice will be highlighted in blue. When you are satisfied that you have selected the correct file, click Open.

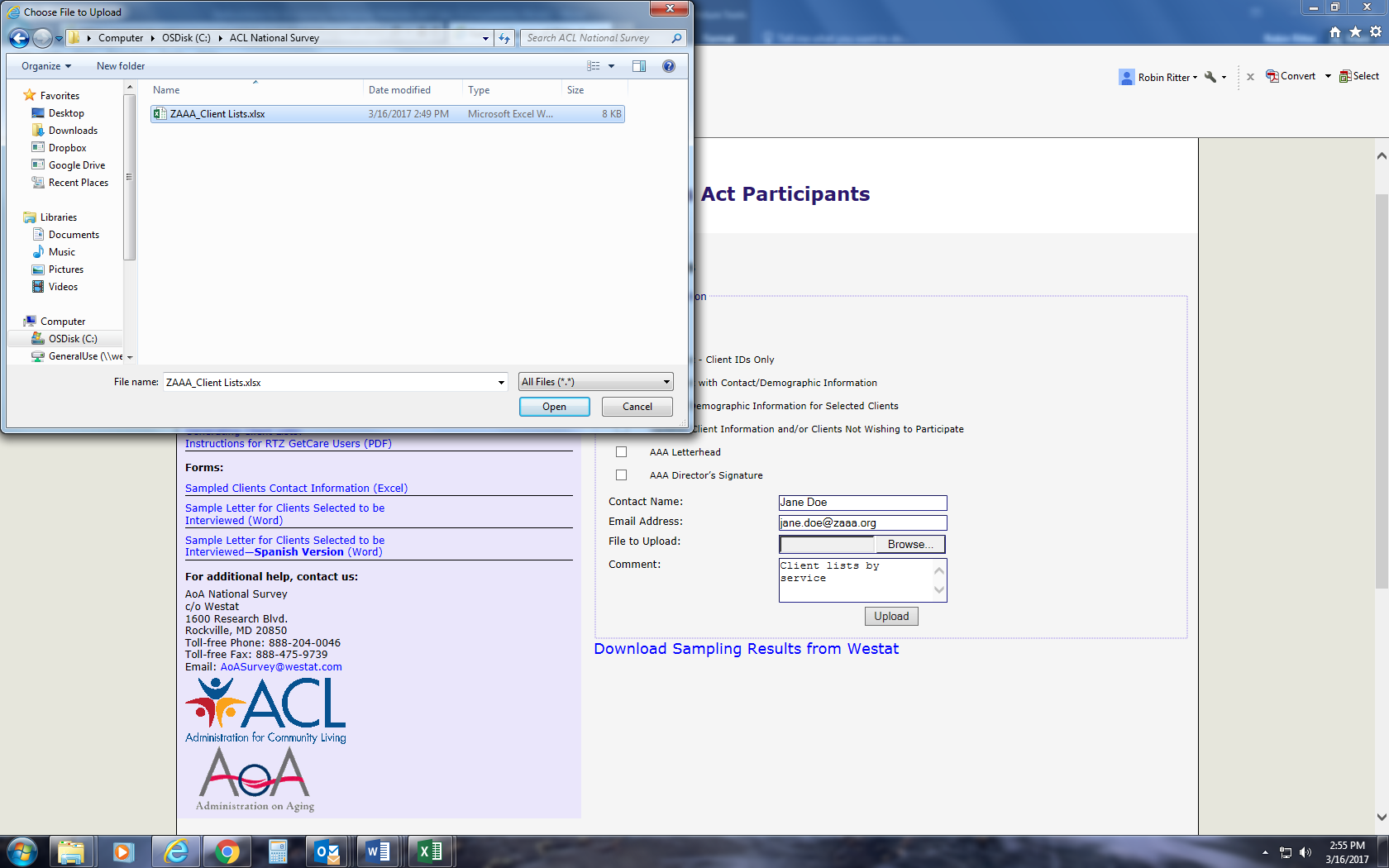
The file that you have selected and opened will appear in the box File to Upload.
If you wish to include any comments, please enter them in the Comment box.
Click Upload and your data will automatically be received by Westat.
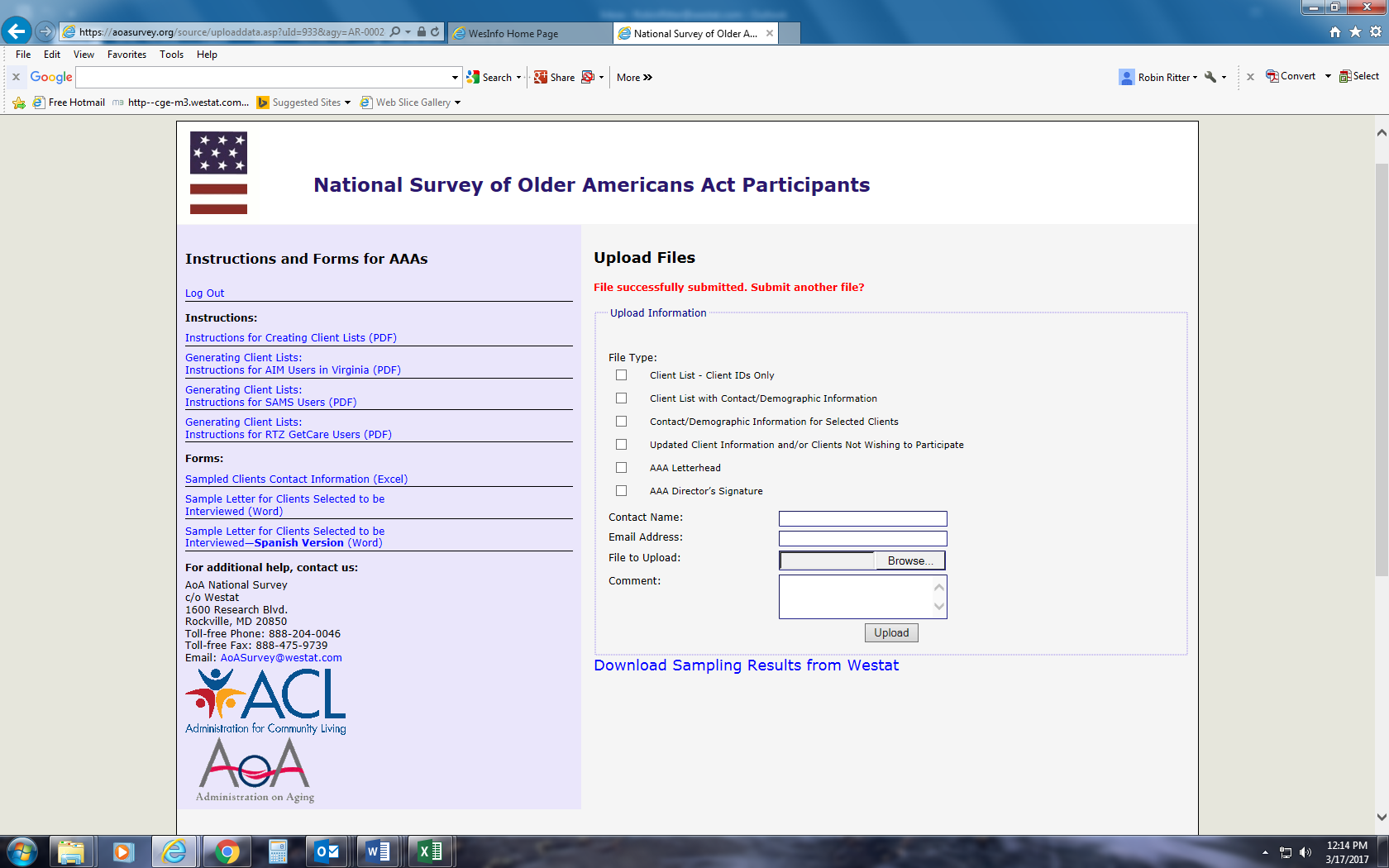
PLEASE NOTE: You can only upload one file at a time. For multiple files, you will have to repeat this process for each separate file.
When the file has been uploaded, you will see a message in red which says,
Files successfully submitted. Select another file?
Step 5: Download sampling results.
If the original client lists that you submitted to Westat contained contact information for all of your clients, Westat will use this information to fill out the Sampled Clients Contact Information form for the clients randomly selected during the sampling procedure. Westat will upload the completed or partially-completed Sampled Clients Contact Information form to your password-protected portion of the website, so that you can download it to your agency’s computer system. We will let you know if additional information is needed on the form.
To download the sampling results provided on a completed or partially-completed Sampled Clients Contact Information form, log into the secure portion of the website using your AAA-ID and password (see Step 2).
On the right-side of the screen, under the Upload Files box, click on the hyperlink that says, Download Sampling Results from Westat.
A new page will open which displays Agency Uploaded Files. The file that Westat has uploaded for your agency has been named for your AAA and is displayed in blue font in the box under the heading that says File Name.
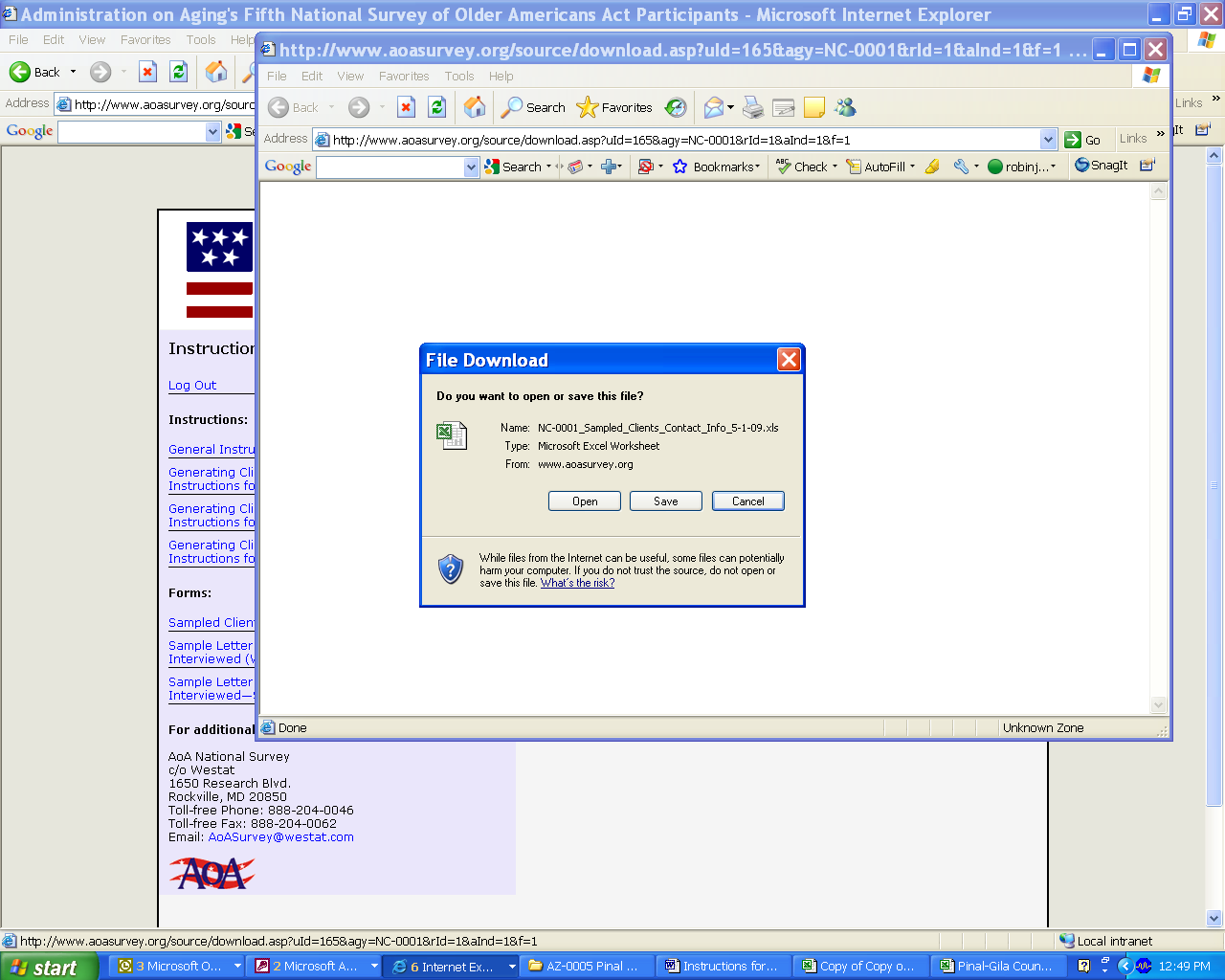
Click on the file name displayed in blue font to open and download the file.
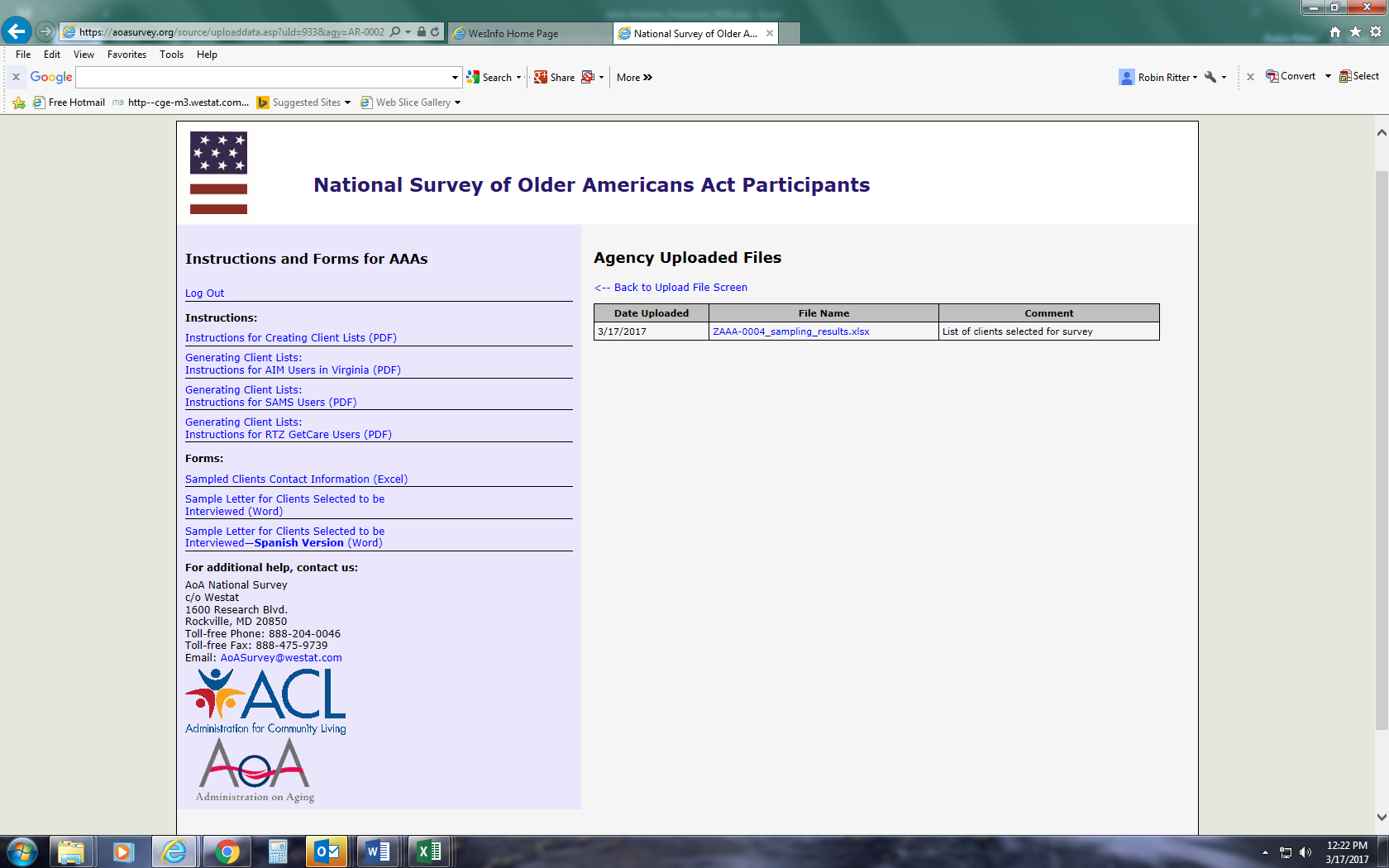
You will see a File Download dialogue box. Save the file to your computer.

The Sampled Clients Contact Information form will show you which clients have been randomly selected for the telephone survey. If your Westat Survey Specialist has asked you for additional information on these clients, please fill in the missing information and resave your file to your computer.
When you have completed filling in the missing information, please upload your completed Sampled Clients Contact Information form to the website (see Step 4-2) and select Client Info for File Type.
Step 6: Log out when you have finished uploading files or downloading sampling results, instructions, and forms.
If at any time you need help with the AoA National Survey website, please contact the AoA National Survey Help Center at 888-204-0062 or by email at AoASurvey@westat.com.
Appendix E
Federal Register Notice
Published by the
Administration for Community Living/
Administration on Aging
for the Proposed Information Collection
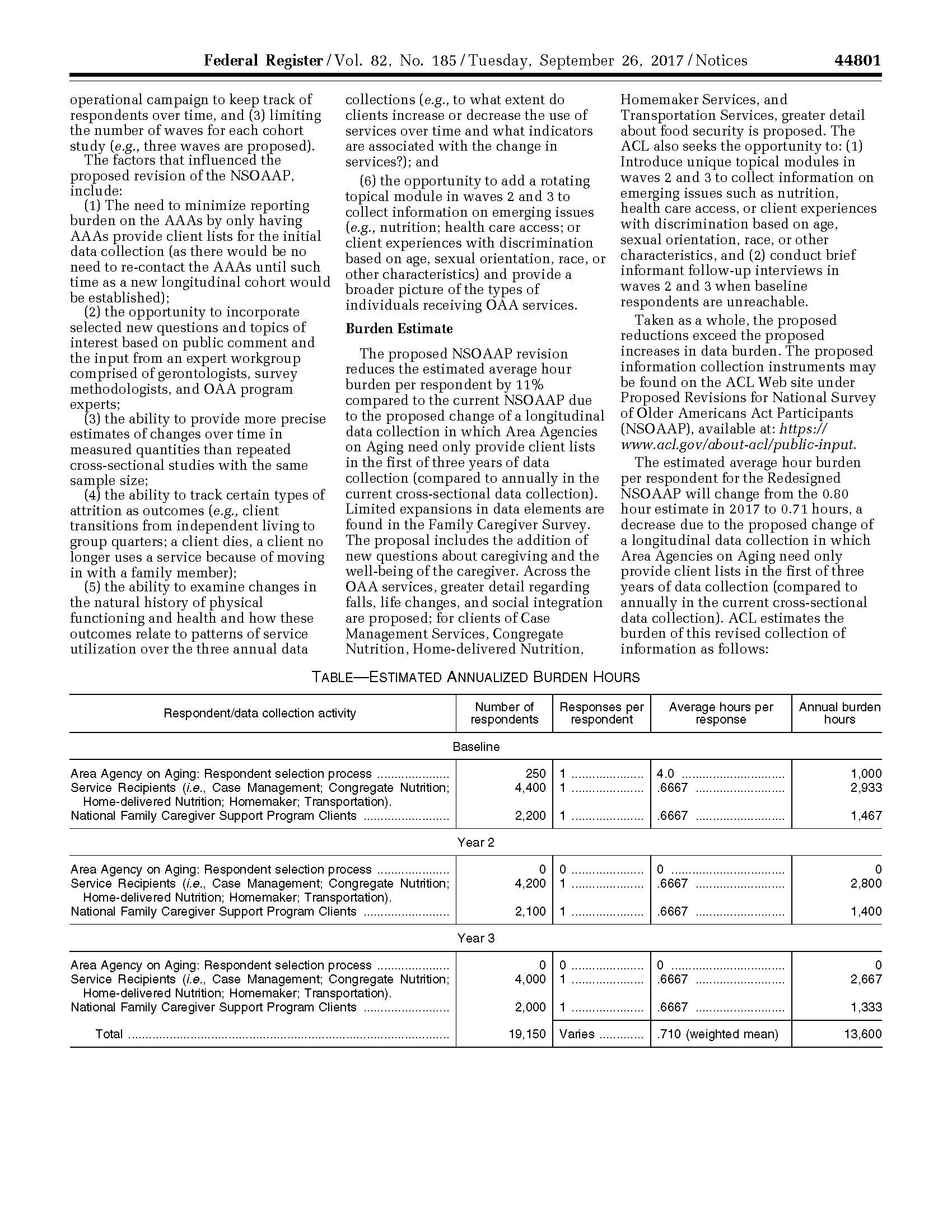
https://www.gpo.gov/fdsys/pkg/FR-2017-09-26/pdf/2017-20460.pdf


Appendix F
Westat Assurance of Confidentiality Agreement
Westat, Inc.
Employee or Contractor’s Assurance of Confidentiality of Survey Data
Statement of Policy
Westat is firmly committed to the principle that the confidentiality of individual data obtained through Westat surveys must be protected. This principle holds whether or not any specific guarantee of confidentiality was given at time of interview (or self-response), or whether or not there are specific contractual obligations to the client. When guarantees have been given or contractual obligations regarding confidentiality have been entered into, they may impose additional requirements that are to be adhered to strictly.
Procedures for Maintaining Confidentiality
1. All Westat employees and field workers shall sign this assurance of confidentiality. This assurance may be superseded by another assurance for a particular project.
2. Field workers shall keep completely confidential the names of respondents, all information or opinions collected in the course of interviews, and any information about respondents learned incidentally during field work. Field workers shall exercise reasonable caution to prevent access by others to survey data in their possession.
3. Unless specifically instructed otherwise for a particular project, an employee or field worker, upon encountering a respondent or information pertaining to a respondent that s/he knows personally, shall immediately terminate the activity and contact her/his supervisor for instructions.
4. Survey data containing personal identifiers in Westat offices shall be kept in a locked container or a locked room when not being used each working day in routine survey activities. Reasonable caution shall be exercised in limiting access to survey data to only those persons who are working on the specific project and who have been instructed in the applicable confidentiality requirements for that project.
Where survey data have been determined to be particularly sensitive by the Corporate Officer in charge of the project or the President of Westat, such survey data shall be kept in locked containers or in a locked room except when actually being used and attended by a staff member who has signed this pledge.
5. Ordinarily, serial numbers shall be assigned to respondents prior to creating a machine-processable record and identifiers such as name, address, and Social Security number shall not, ordinarily, be a part of the machine record. When identifiers are part of the machine data record, Westat’s Manager of Data Processing shall be responsible for determining adequate confidentiality measures in consultation with the project director. When a separate file is set up containing identifiers or linkage information which could be used to identify data records, this separate file shall be kept locked up when not actually being used each day in routine survey activities.
6. When records with identifiers are to be transmitted to another party, such as for keypunching or key taping, the other party shall be informed of these procedures and shall sign an Assurance of Confidentiality form.
7. Each project director shall be responsible for ensuring that all personnel and contractors involved in handling survey data on a project are instructed in these procedures throughout the period of survey performance. When there are specific contractual obligations to the client regarding confidentiality, the project director shall develop additional procedures to comply with these obligations and shall instruct field staff, clerical staff, consultants, and any other persons who work on the project in these additional procedures. At the end of the period of survey performance, the project director shall arrange for proper storage or disposition of survey data including any particular contractual requirements for storage or disposition. When required to turn over survey data to our clients, we must provide proper safeguards to ensure confidentiality up to the time of delivery.
8. Project directors shall ensure that survey practices adhere to the provisions of the U.S. Privacy Act of 1974 with regard to surveys of individuals for the Federal Government. Project directors must ensure that procedures are established in each survey to inform each respondent of the authority for the survey, the purpose and use of the survey, the voluntary nature of the survey (where applicable) and the effects on the respondents, if any, of not responding.
PLEDGE
I hereby certify that I have carefully read and will cooperate fully with the above procedures. I will keep completely confidential all information arising from surveys concerning individual respondents to which I gain access. I will not discuss, disclose, disseminate, or provide access to survey data and identifiers except as authorized by Westat. In addition, I will comply with any additional procedures established by Westat for a particular contract. I will devote my best efforts to ensure that there is compliance with the required procedures by personnel whom I supervise. I understand that violation of this pledge is sufficient grounds for disciplinary action, including dismissal. I also understand that violation of the privacy rights of individuals through such unauthorized discussion, disclosure, dissemination, or access may make me subject to criminal or civil penalties. I give my personal pledge that I shall abide by this assurance of confidentiality.
________________________________________
Signature
_________________________________________
Printed Name
_________________________________________
Date
Appendix G
Agency Information Packet:
1. Letter to Area Agencies on Aging
2. Memo and Sampling Instructions
3. Pre-notification Client Information Letter
4. Sampled Client Contact Information Form

May 1, 2017
«Title» «AAA__Director_First_Name» «AAA__Director__Last_Name»
«AAA_Name»
«Address_1», «Address_2»
«City», «State» «ZIP»
Dear «Title» «AAA__Director__Last_Name»:
The Administration for Community Living (ACL) is undertaking a three-year longitudinal study of Older Americans Act Participants. Your agency has been randomly selected to participate along with approximately half of the other AAAs in the 50 states and the District of Columbia.
Your cooperation is essential to the success of this survey. The NLSOAAP provides ACL with an effective method for collecting timely data to meet the accountability requirements of Congress and the executive branch of the federal government. The results of this survey can also be used for your own advocacy and business purposes.
ACL would like to contact a sample of older adults served by your organization for the national survey. The NLSOAAP will determine consumer assessment of the services they receive, as well as outcomes of those services for participants. The survey results will demonstrate to the President, Congress, and other decision makers the outstanding outcomes that the aging network produces. Powerful information from surveys is used for performance outcome measures, to support ACL budget requests, and to enhance our continued pursuit of support for long term care services and supports (LTSS). Performance measurement is critical to improving LTSS for all consumers.
As required, ACL requested and received approval from the Office of Management and Budget (OMB) to identify and to survey elderly individuals and family caregivers who receive OAA services (OMB approval number is XXXXX-XXXX. The approval covers the sampling of area agencies on aging and their clients, and conducting surveys to assess the following service categories: congregate and home-delivered meals, caregiver, case management, homemaker, and transportation services.
We are asking for your assistance in selecting service recipients to be interviewed for the survey. The enclosed instructions describe the steps to help us select these participants. All participant responses will be kept private and the analysis will not be linked with either individuals or your agency. We anticipate the development of client lists to be used to select the survey participants will take you less than two hours to complete. You will be working with Robin Ritter and her staff from Westat to complete this procedure. If you have any questions, you may contact the Westat National Survey specialists at 1-888-204-0046 or by email at aoasurvey@westat.com.
To communicate the importance of the survey and to explain the logistics involved, ACL and Westat are holding a kick-off webinar event for SUAs and AAAs on XXXX at 1:30 pm EDT. Please see the enclosed webinar invitation for further information. The webinar will be recorded and will be available to replay, if you are not available at that time.

«Title» «AAA__Director_First_Name» «AAA__Director__Last_Name»
May 1, 2017
Page 2
Unlike the previous years, the NLSOAAP is now a three-year longitudinal study. We will interview the sampled clients at baseline, year 2 and year 3. This means that your agency will not be asked to sample clients again during the second and third years of the study period.
If you have any questions about your participation in the survey, please call ACL at 1-888-204-0271. On behalf of the Administration for Community Living, U.S. Department of Health and Human Services, I would like to thank you for your assistance in this project. Your help is invaluable for the completion of this study.
Sincerely,

Susan Jenkins, PhD
Director, Office of Performance and Evaluation
Center for Policy and Evaluation
cc: SUA Director; ACL Regional Administrator


An Employee-Owned Research Corporation

MEMORANDUM
DATE: |
<DATE> |
|
|
TO: |
|
|
|
FROM: |
Robin Ritter, Manager of Survey Operations |
|
|
SUBJECT: |
National Longitudinal Survey of Older Americans Act Participants |
Westat is conducting a three-year longitudinal survey of Older Americans Act Participants for the Administration for Community Living, U. S. Department of Health and Human Services. Your Agency was selected as part of a representative sample of all Area Agencies on Aging in the United States, and your participation is essential for the success of this study.
You will be assisting ACL by providing information that will allow Westat, ACL’s contractor, to survey individual clients and caregivers who receive OAA services. We will work with your staff to randomly select clients and caregivers to take part in a telephone interview to assess OAA programs. The data collected from the survey will be used to document the outcomes of services provided by the Aging Network.
Services that are being evaluated include:
Case Management
Congregate Meals
Home Delivered Meals
Homemaker Services
Transportation Services
National Family Caregiver Support Program
Enclosed you will find instructions on how clients will be randomly selected for the survey and your agency’s role in that process. If you have any questions or concerns, please do not hesitate to contact us:
By telephone: 1-888-204-0046 (toll free)
By email: AoAsurvey@westat.com.
We are looking forward to working with you and your staff, and we are committed to making this study as efficient and effective as possible. Thank you for your participation.
Contents Page
Letter from the Administration for Community Living
Memo from Westat 1
Summary of AAA Responsibilities 2
Instructions for Creating Client Lists (Checklist) 3
Detailed Instructions for the ACL/AoA National Longitudinal Survey of OAA Participants 5
Older Americans Act Title III Service Definitions 9
Sample Letter for Clients Selected to be Interviewed 12
Login & Password/Instructions for Accessing the AoA National Survey Website
Summary of AAA Responsibilities for the
Baseline ACL/AoA National Longitudinal Survey
Summary of Responsibilities of the AAA Executive Director:
Please designate a person within your agency to be a survey liaison or point-of-contact with whom we will work to gather and complete the necessary client lists and client contact information.
Please provide us with the contact person’s name, email address, and phone number in an email message to our secure mailbox: aoasurvey@westat.com or call us at 1-888-204-0046.
Summary of Responsibilities of the AAA’s Survey Liaison:
Step 1: Generate separate lists of active OAA clients by service. Six services are being studied this year and are outlined further on in this memo.
Step 2: Upload the service lists to the AoA Survey secure website. Westat staff will use a special computer program to randomly select clients from your service lists who will be interviewed for the study, and we will inform you of the specific clients selected.
Step 3: Provide Westat staff with contact information for those clients selected to be interviewed. Forms (Excel) for recording the contact information for the clients selected to be interviewed can be downloaded from the AoA National Survey website https://aoasurvey.org/default.asp or you may use your own spreadsheets, provided that the required contact information is included for each client.
Step 4: Notify the clients selected to be interviewed about the study. A sample letter is provided in this packet; you can also download a copy of this sample letter from the AoA National Survey website https://aoasurvey.org/default.asp. To save time and the cost of postage, Westat can create and mail the letter for you on your AAA’s letterhead, if desired.
Step 5: Notify Westat of any clients who do not wish to participate or whose contact information has changed. More detailed instructions are included on the pages following this section. Your Westat Survey Specialist will work with you to accommodate scheduling concerns, data format issues, or any other problems you might foresee or encounter.
Instructions for Creating Client Lists
Generate separate lists of active Older Americans Act Title III clients by type of service received using your client tracking software using either the one-step or two-step method.
One-step method: Generate separate lists (separate Excel worksheet tabs or files) of clients by service and include all client contact information needed for clients selected to be interviewed (see chart on next page).
Upload separate service lists to AoA Survey website https://aoasurvey.org/source/login.asp.
Westat survey specialists will use a specialized computer program to randomly select a small number of clients per service to be interviewed.
Westat will notify AAA of the clients that were selected by uploading list of selected clients to the AAA’s secure portion of the AoA Survey website.
Westat will destroy client contact information for any clients who were not selected to be interviewed.
Client contact information for clients selected to be interviewed will be used to send the informed consent letters and to contact the clients for their interviews; all client contact information will be destroyed by 12/31/14.
Two-step method:
Step 1: Generate separate lists of clients by service using client IDs only.
Upload separate service lists to AoA Survey website https://aoasurvey.org/source/login.asp.
Westat survey specialists will use a specialized computer program to randomly select a small number of clients per service to be interviewed and will notify AAA of the client IDs that were selected.
Step 2: Provide detailed client contact information for the client IDs that were randomly selected (see chart on next page).
Upload client contact information on the Sampled Clients Contact Information form (Excel) or alternate Excel format.
Client contact information for clients selected to be interviewed will be used to send the informed consent letters and to contact the clients for their interviews; all client contact information will be destroyed by 12/31/14.
Things to consider regardless of which method you use to create your client lists for sampling:
Each list should consist of clients who have received the OAA services during the most recent 12 month period.
Before you select your lists of clients, if possible, select clients who are CURRENTLY ACTIVE; please do not include any clients who are known to be deceased or have moved out of the area.
Each client who received the service will need to be listed on a separate line. Clients can be represented by a client ID (not a Social Security Number).
For the five (5) non-caregiver services, the following information is needed for each client selected to be interviewed:
Case Management |
Congregate Meals |
Home-Delivered Meals |
Homemaker |
Transportation |
OAA Title III-B |
Title III-C1 |
Title III-C2 |
Title III-B |
Title III-B |
Clients age 60+ |
Clients age 60+ |
Clients age 60+ |
Clients age 60+ |
Clients age 60+ |
Client Name |
Client Name |
Client Name |
Client Name |
Client Name |
Client Phone |
Client Phone |
Client Phone |
Client Phone |
Client Phone |
Client DOB |
Client DOB |
Client DOB |
Client DOB |
Client DOB |
Client Gender |
Client Gender |
Client Gender |
Client Gender |
Client Gender |
Client Address |
Client Address |
Client Address |
Client Address |
Client Address |
Client City |
Client City |
Client City |
Client City |
Client City |
Client State |
Client State |
Client State |
Client State |
Client State |
Client Zip Code |
Client Zip Code |
Client Zip Code |
Client Zip Code |
Client Zip Code |
Service Provider |
Service Provider |
Service Provider |
Service Provider |
Service Provider |
For Family Caregiver services, the following information is needed for each client selected to be interviewed:
National Family Caregiver Support Program
|
Title III-E clients who receive any of the following: Counseling and Support, Respite Services, and Supplemental Services (I&A and Grandparents Caring for Grandchildren are excluded) |
Caregiver Name (persons providing care for persons age 60 years and older) |
Caregiver Phone |
Caregiver Date of Birth |
Caregiver Gender |
Caregiver Address |
Caregiver City |
Caregiver State |
Caregiver Zip Code |
Service Provider |
Care Recipient Name (Persons receiving care age 60 or older) |
Care Recipient Date of Birth (Age 60 or older) |
Care Recipient Gender |
Detailed Instructions for the
Baseline ACL/AoA National Longitudinal Survey of OAA Participants
Generate separate numbered lists of OAA clients by type of service received using your client tracking software. Instructions for creating numbered client lists for Virginia’s version of AIM or PeerPlace are included in this packet. Please refer to the “Instructions for Creating Client Lists” on pages 3-4 to determine if you wish to use the “one-step” or “two-step method.” Each list should consist of clients who have received the following services during the most recent 12 month period. Note: before you select your lists of clients, please do not include any clients who are known to be deceased or have moved out of the area. Each client who received the service will need to be listed on a separate row. You will need to have six separately numbered lists for each of the following:
Case Management
Congregate Meals
Home-delivered Meals
Homemaker Services
Transportation Services (Please do not include clients who receive assisted transportation services.)
Caregivers caring for care recipients age 60 or older who received any of the following services through the National Family Caregiver Support Program (except those who received information and assistance services only):
Individual counseling, participation in support groups, and/or caregiver training to assist the caregivers in making decisions and solving problems relating to their caregiving roles
Respite care to enable caregivers to be temporarily relieved from their caregiving responsibilities
Supplemental services, on a limited basis, to complement the care provided by caregivers.
Please do not include caregivers who have received information and assistance services only, and please do not include grandparents caring for grandchildren or anyone caring for individuals who are less than 60 years old.
Upload the service lists to the AoA Survey secure website.
Upload your file(s) containing your numbered client lists by service to the AoA National Survey secure website https://aoasurvey.org/default.asp. You will be required to log-in with your unique AAA-ID or SUA-ID and password, and provide the name of the person uploading the file.
Your Westat Survey Specialist will enter your client service list totals into a special computer program which will randomly select clients by row numbers from each of your numbered lists. The randomly selected row numbers indicate the client IDs or client names selected for the survey.
If you use the two-step method and submit service lists with client IDs only, your Westat Survey Specialist will provide you with the sampling results showing the specific client IDs representing the clients selected to be interviewed for the survey. You will then need to provide Westat with the client names and contact information that corresponds to the selected client IDs.
If you use the one-step method and submit service lists with all client names and contact information included in advance, your Westat Survey Specialist will upload the sampling results to your AAA secure portion of the AoA survey website. The sampling results will list the specific clients selected to be interviewed for the survey; all non-selected clients will have been deleted. You can disregard Step 3 below and move to Step 4 (notify selected clients).
If you used the two-step method and submitted only client IDs, you will need to provide Westat with client names and contact information for only those clients IDs selected on the random sampling report. You can use the Sampled Clients Contact Information Form (an Excel file) to record client contact information; the form can be downloaded from the AoA National Survey secure website https://aoasurvey.org/default.asp. If you prefer, you can use an alternate Excel format of your choice as long as it contains the required contact information for each client.
For Care Management, Congregate Meals, Home Delivered Meals, Homemaker Service, and Transportation, the following information is needed for each client selected to be interviewed:
Client name (Last Name; First Name)
Client telephone number
Client date of birth
Client gender
Client address
Service Provider
Any accommodations, if known, that the client would need to complete the telephone survey. A proxy (usually a relative or a caregiver) may be designated to answer the survey questions on the client’s behalf due to speech, language, hearing, cognitive or other difficulties. Similarly, an interpreter may be designated to answer the survey questions for non-English speaking clients.
For Caregivers, the following information is needed for each Caregiver selected to be interviewed
Caregiver name
Client telephone number
Caregiver date of birth
Caregiver gender
Caregiver address
Any accommodations, if known, that the caregiver would need to complete the survey (e.g., a proxy or an interpreter may be designated to answer the survey questions on the caregiver’s behalf due to speech, language, hearing, or other difficulties or for non-English speaking caregivers).
For caregivers, we are also asking for the name, date of birth, and gender of the person they are caring for (if the information is available).
Provide Westat with the contact information for the clients and caregivers by one of the following methods ranked in order of most secure:
Upload the completed Sampled Clients Contact Information Form or other file containing client contact information to the AoA National Survey secure website https://aoasurvey.org/default.asp.
If you experience difficulty using the secure website, you can send the information via email to the secure email account: aoasurvey@westat.com. If selecting this method, please password-protect your file and send the password to Westat in a separate email message.
Send the information to Westat by Federal Express (Westat will provide you with prepaid Federal Express shipping labels when requested):
Westat
ATTN: Robin Ritter
1600 Research Blvd
RW 3658
Rockville, MD 20850
Fax the information to: 888-475-9739 (toll-free).
We would like to have this process completed by June 30, 2017, if possible.
Notify the clients selected to be interviewed about the study and the importance of their participation. A sample informed consent letter is provided in this packet; you can also download the Sample Letter to Notify Clients Selected to be Interviewed as a Word file from the AoA National Survey website https://aoasurvey.org/default.asp. A separate Spanish language version of the letter can also be downloaded from the website. Please send each client who was selected a letter requesting his/her participation in the study using your agency’s letterhead. This will let your clients know that this is a legitimate telephone survey and how important the study is. Please check with your Westat Survey Specialist for guidance on when to mail the letter. Alternatively, Westat can mail the client letters for your agency if you provide us with your agency letterhead. You can upload Word or jpg files containing your letterhead and executive director’s signature to the AoA National Survey secure website.
Notify Westat of any clients who do not wish to participate, are unable to participate, or whose contact information has changed. After receiving the letter, if a client notifies you that they do not want to participate or you find that they are no longer able to participate (moved, nursing home placement, death), please upload the updated client information to the AoA National Survey website or notify your Westat Survey Specialist, and we will remove the client’s name and contact information from our lists of clients to be called for the survey. Otherwise, telephone interviews are scheduled to start the week of July 15, 2017 and will continue into October.
Older Americans Act Title III Service Definitions
Case Management (Title III B)
A client-centered service providing assistance in the form of care coordination or access
Activities include needs assessment; care plan development and implementation; case coordination (authorizing and arranging for services, coordinating the provision of services among providers); follow-up and reassessment of client status.
Homemaker Services (Title III B)
Homemaker services provide assistance with specific home management duties for persons having difficulty with one or more of the following instrumental activities of daily living (IADL): preparing meals, managing money, shopping for groceries or personal items, performing light or heavy housework, and using a telephone.
Transportation (Title III B)
Providing transportation to or from health and medical care, community services, recreational activities, and shopping
Eligible clients are those who have difficulties (physical or cognitive) using regular transportation.
Congregate Meals/Congregate Nutrition Services (Title III C-1)
The provision of a meal at a congregate meal site
Home Delivered Meals (Title III C-2)
A meal delivered to the home of an eligible client or other eligible participant
National Family Caregiver Support Program (Title III E)
For this study, a Family Caregiver participant in the National Family Caregiver Support Program is defined as an individual who is providing care for another adult family member 60 years of age or over in the home. The person for whom the Family Caregiver provides care for is the “Care Recipient.” Although the Care Recipient may receive other OAA services provided by the AAA, it is the Caregiver who provides care that is the focus of the Caregiver section of this study.
Registered Services:
Counseling: Provide individual counseling, organization of support groups, and caregiver training to family caregivers on an individual or group basis.
Respite Care: Provide temporary, substitute care arrangements to provide a brief period of rest or relief for family caregivers.
Supplemental Services: Services to complement the care provided by family caregivers such as emergency medical transportation not covered by insurance and other activities; home modifications not covered under Title IIIB, Medicare or other insurance
Please note the following exceptions for National Family Caregiver Support Program (Title III E):
Grandparents or other older individuals providing care for individuals less than 60 years of age are not eligible for this study and should not be included on client lists.
Information & Assistance for caregivers about available services is not included in this study. For this study, we are limiting the Caregiver survey to persons who are receiving registered Family Caregiver services (Counseling, Respite Care, and Supplemental Services). Although many individuals may also be receiving Information and Assistance (I&A), if I&A is the only service that they have received, they should not be included in the client lists for the survey.
Sources:
National Family Caregiver Support Program https://www.acl.gov/node/314
Older Americans Act https://www.acl.gov/about-acl/authorizing-statutes/older-americans-act
Sample Letter for Clients Selected to be Interviewed
Tri-County Area Agency on Aging
123 Anywhere St.
Anywhere, XX 12345
<DATE>
Dear Mr./Mrs. ______________________________ ,
We are writing to ask for your help. <<INSERT AAA NAME>> is taking part in a study for the Administration for Community Living (ACL)/Administration on Aging (AoA), part of the U.S. Department of Health and Human Services. ACL/AoA wants to know what people around the country think about the meal programs, transportation, family caregiver, and other services offered by their local AAA.
You have been chosen to be part of this national three-year study. An interviewer from Westat, a research firm working for AoA, will call you in the near future to ask you some questions about your experience with <<INSERT AAA NAME & PROVIDER NAME IF KNOWN>>. Your answers will be kept private. Your name won’t be given to anyone else. The interviewer will also call you a year from now to conduct an interview, and two years from now to interview you again.
Your answers will be combined with answers from other clients and will be part of a report to Congress about how well these services are meeting the needs of older Americans. AoA and Congress will use this information to help them decide how well the programs are working and what improvements to make. Your answers will be very important in helping AoA and Congress decide what to do.
I hope you will be part of this important study. It’s your choice. Whatever you decide, it won’t affect the services you get now or in the future. If you do not want to take part in this study, please call <<INSERT AAA CONTACT NAME>> at <<INSERT AAA PHONE NUMBER>> by <<INSERT DATE>>.
If you have any questions about this study, please call Westat toll-free at 1-888-204-0046 or the Administration on Aging toll-free at 1-888-204-0271. If you have any questions about the services you get, please call our office at <<INSERT AAA PHONE NUMBER>>.
Thank you for your help and support.
Sincerely,
______________________________,
Executive Director
An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. The OMB control number for this information collection is XXXX-XXXX. Public reporting burden for this information collection is estimated to average 35 minutes per response; response times may range from 20 minutes to 40 minutes. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to the Administration for Community Living/Administrate
Appendix H
Reminder Card
<DATE>
Dear Survey Participants:
Thank you for participating in this important survey about the services you receive from [Agency XYZ]. As we mentioned when you participated a year ago, Westat will interview you again in the coming months about the services you have received since then. The information you provide helps ACL/AoA find out about how you feel about the services. This information helps ACL/AoA ensure the quality of the services and provides information for justifying budget requests to Congress.
We sincerely hope you will participate in this second interview. Your participation is vital to helping ACL/AoA understand how your thoughts about services have changed over the past year.
The charts on the back of this page show information that you have helped us collect.
Sincerely yours,
Susan Jenkins, PhD
Director, Office of Performance and Evaluation
Center for Policy and Evaluation
Appendix I
Follow-up Survey
Telephone Script
Introduction
I am calling from Westat, a research firm that is conducting the National Survey of Older Americans Act Participants funded by the Administration for Community Living/Administration on Aging. The survey is about the services that [NAME OF PARTICIPANT]1 receives from [AGENCY NAME]. We have been unable to reach [NAME OF PARTICIPANT]. [He/she] participated in an earlier interview with Westat, and gave me your contact information in case we could not reach [him/her]. We have been unable to reach [NAME OF PARTICIPANT] and want to ask you a few questions about how to reach [him/her.]
A. RELATIONSHIP TO RESPONDENT IN THE LONGITUDINAL SURVEY
First, I need to verify your relationship to {NAME OF PARTICIPANT}.
A1. What is {you/his/her} relationship to {NAME OF PRTICIPANT}? Are you {his/her}...
HUSBAND, 1
WIFE, 2
SON, 3
SON-IN-LAW, 4
DAUGHTER, 5
DAUGHTER-IN-LAW, 6
FATHER, 7
MOTHER, 8
BROTHER, 9
SISTER, 10
GRANDDAUGHTER, 11
GRANDSON, 12
NIECE, 13
NEPHEW, 14
A FRIEND OR NEIGHBOR OR ANOTHER PERSON,
OR 15
OTHER RELATIVE 91
(SPECIFY)
REFUSED -7
DON’T KNOW -8
A2. When was the last time you spoke to {NAME OF PARTICIPANT} either by phone or in-person?
|___|___| / |___|___|
Month Year
IF MORE THAN ONE MONTH GO TO A3; ELSE GO TO A4.
In order to complete our records that we are unable to reach [NAME OF PARTICIPANT], I would like to ask the reason you are unable to reach {him/her}.
A3. What are the reasons that you have not had much contact with (NAME OF PARTICIPANT)?
PARTICIPANT DIED 1 GO TO C
PERSON HAS A PHYSICAL LIMITATION
(E.G., HEARING LOSS, VISION, LOSS, ETC.) 2
PARTICIPANT MOVED 3
OTHER -9
(SPECIFY)
A4. Please tell me how I may contact {NAME OF PARTICIPANT}?
Phone #
Address:
A5. Would {NAME OF PARTICIPANT} be able to respond to the survey?
YES 1 GO TO CLOSING
NO 2
REFUSED -7
DON’T KNOW -8
CLOSING: Thank you very much for your time. I will contact [name of participant] directly.
B. RECEIPT OF SERVICES
Since {NAME OF PARTICIPANT} is unable to answer questions for {himself/herself}, I would like to ask you a few questions. {NAME OF PARTICIPANT} agreed to answer these and other questions when we last spoke to {him/her}. The questions are about the services {he/she} received, {his/her} physical functioning, and health conditions. It will only take about 10 minutes for me to ask you the questions. Your participation is voluntary and you may skip any question that you do not want to answer. Your answers will be combined with the answers from other survey participants. The information you give me will only be seen by the research team, and will not be shared with anyone else. The information we collect from you and any other study participants will give the Administration for Community Living/Administration on Aging information on how well the services are working. May I continue?
B1. Is {NAME OF PARTICIPANT} still receiving services from [AGENCY NAME]?
YES 1 GO TO SECTION E
NO 2


GO TO B1a
REFUSED -7
DON’T KNOW -8
B1a. If “No,” when did {NAME OF PARTICIPANT} stop receiving services?
|___|___| / |___|___| / |___|___|___|___|
Month Day Year
B1b. If “No,” why did the respondent stop receiving services?

A. MOVED TO ANOTHER LOCATION IN THE
COMMUNITY OR OUT OF THE AREA 1
B. MOVED TO A NURSING HOME BECAUSE OF
ILLNESS/INJURY 2
B. MOVED TO BE CLOSER TO RELATIVES 3
C. MOVED TO ASSISTED LIVING BECAUSE OF GO TO SECTION E
ILLNESS/INJURY 4
D. MOVED TO GROUP HOME, BOARD AND
CARE HOME, ETC. BECAUSE OF ILLNESS/INJURY 5
E. MOVED IN WITH A FRIEND OR RELATIVE
BECAUSE OF ILLNESS OR INJURY 6


GO TO SECTION D
F. RECEIVING SERVICES FROM ANOTHER AGENCY 7
G. HAS A PRIVATE CAREGIVER IN THE HOME 8

H. IN HOSPICE (IN HOME OR IN A FACILITY) 9
I. DISSATISFIED WITH THE SERVICE 10
GO TO SECTION E
J. OTHER? 91
(SPECIFY)
REFUSED -7
DON’T KNOW -8
C. PARTICIPANTS WHO ARE NO LONGER LIVING
C1. What is [NAME OF RESPONDENT] date of death?
|___|___| / |___|___|___|___|
Month Year
C2. Where was [NAME OF RESPONDENT] living at the time of death?
OWN HOME 1
RELATIVES HOME 2
HOSPICE 3
NURSING HOME 4
ASSISTED LIVING 5
GROUP HOME 6
REFUSED -7
DON’T KNOW -8
Somewhere else -9
SPECIFY
CLOSING 1: Thank you very much for answering my questions.
D. RESPONDENT RECEIVES SERVICES FROM ANOTHER AGENCY
We would like to learn more about the types of services that [NAME OF PARTICIPANT} receives. The next few questions ask about [him/her] receiving services from another agency.
D1. What was the reason {NAME OF PARTICIPANT} switched to another agency?
D2. Does {NAME OF PARTICIPANT} receive the same type of services as {he/she} did from [AGENCY NAME]?
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
D2a. If “No,” please describe services received from the new agency.
E. ACTIVITIES OF DAILY LIVING
The next few questions are about {NAME OF PARTICIPANT}. To the best of your ability, please answer the following questions.
E1. Does {NAME OF PARTICIPANT} have difficulty getting around inside the home?
(PFDFINC)
YES 1

NO 2
REFUSED -7 GO TO E2
DON’T KNOW -8
E1a. {Does s/he} need the help of another person to perform this activity?
(PFDFINBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E2. Does {s/he} have difficulty going outside the home, for example to shop or visit a doctor’s office?
(PFDFOUC)
YES 1

NO 2
REFUSED -7 GO TO E3
DON’T KNOW -8
E2a. Does {s/he} need the help of another person to perform this activity?
(PFDFOUBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E3. Does {NAME OF PARTICIPANT} have difficulty getting in or out of bed or a chair?
(PFBEDC)
YES 1
NO 2
REFUSED -7 GO TO E4
DON’T KNOW -8
E3a. Does {s/he} need the help of another person to perform this activity?
(PFBEDBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E4. Does {s/he} have difficulty when taking a bath or shower?
(PFBATHC)
YES 1
NO 2
REFUSED -7 GO TO E5
DON’T KNOW -8
E4a. Does {s/he} need the help of another person to perform this activity?
(PFBATHBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E5. Does {NAME OF PARTICIPANT} have difficulty when dressing?
(PFDRESC)
YES 1
NO 2
REFUSED -7 GO TO E6
DON’T KNOW -8
E5a. Does {s/he} need the help of another person to perform this activity?
(PFDRESBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E6. Does {s/he} have difficulty when walking?
(PFWALKC)
YES 1
NO 2
REFUSED -7 GO TO E7
DON’T KNOW -8
E6a. Does {s/he} need the help of another person to perform this activity?
(PFWALKBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E7. Does {NAME OF PARTICIPANT} have difficulty eating?
(PFEATC)
YES 1
NO 2
REFUSED -7 GO TO E8
DON’T KNOW -8
E7a. Does {s/he} need the help of another person to perform this activity?
(PFEATBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E8. Does {s/he} have difficulty using the toilet or getting to the toilet?
(PFWCC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
E8a. Does {s/he} need the help of another person to perform this activity?
(PFWCBC)
YES 1
NO 2
REFUSED -7
DON’T KNOW -8
F. Health Conditions
PROGRAMMER NOTE:
JUST DISPLAY CONDITIONS PREVIOUSLY CODED AS “NO.”
F1. Now I would like to ask about medical conditions [NAME OF PARTICIPANT] may have. Has a doctor ever told [NAME OF PARTICIPANT] that {s/he has} had:
(PFDISA - PFDISU) |
YES |
NO |
RF |
DK |
N/A |
a. Arthritis or rheumatism? |
1 |
2 |
-7 |
-8 |
-9 |
b. High blood pressure or hypertension? |
1 |
2 |
-7 |
-8 |
-9 |
c. A heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems? |
1 |
2 |
-7 |
-8 |
-9 |
d. High cholesterol? |
1 |
2 |
-7 |
-8 |
-9 |
e. Diabetes or high blood sugar? |
1 |
2 |
-7 |
-8 |
-9 |
f. Allergies/asthma/emphysema/chronic bronchitis/other breathing and lung problems? |
1 |
2 |
-7 |
-8 |
-9 |
g. Cancer or a malignant tumor, excluding minor skin cancer? |
1 |
2 |
-7 |
-8 |
-9 |
h. Stroke? |
1 |
2 |
-7 |
-8 |
-9 |
i. Anemia? |
1 |
2 |
-7 |
-8 |
-9 |
j. Osteoporosis? |
1 |
2 |
-7 |
-8 |
-9 |
k. Kidney disease? |
1 |
2 |
-7 |
-8 |
-9 |
l. Eye or vision conditions such as glaucoma, cataracts, macular degeneration or other medical conditions? |
1 |
2 |
-7 |
-8 |
-9 |
INTERVIEWER NOTE: This does not include only wears glasses or contacts. |
|||||
m. Hearing problems? |
1 |
2 |
-7 |
-8 |
-9 |
n. Emotional, nervous or psychiatric problems? |
1 |
2 |
-7 |
-8 |
-9 |
o. Memory related disease such as Alzheimer’s or dementia? |
1 |
2 |
-7 |
-8 |
-9 |
p. Seizures or epilepsy? |
1 |
2 |
-7 |
-8 |
-9 |
q. Parkinson’s? |
1 |
2 |
-7 |
-8 |
-9 |
r. Persistent pain, aching, stiffness or swelling around a joint? |
1 |
2 |
-7 |
-8 |
-9 |
INTERVIEWER NOTE: Includes broken BONES; sprained muscles; bad backs, knees, shoulders, etc. |
|||||
s. Multiple sclerosis? |
1 |
2 |
-7 |
-8 |
-9 |
t. A serious problem with urinary incontinence? |
1 |
2 |
-7 |
-8 |
-9 |
u. Something else? (SPECIFY) __________________________________________ |
1 |
2 |
-7 |
-8 |
-9 |
CLOSING 2: That is all the questions that I have for you today. Thank you very much for answering the questions.
1 [NAME OF PARTICIPANT] IS THE PERSON SAMPLED FOR THE LONGITUDINAL NSOAAP
A-
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | NSOAAP Appendices |
| Author | Beth Rabinovich |
| File Modified | 0000-00-00 |
| File Created | 2021-01-15 |
© 2026 OMB.report | Privacy Policy