2 Part 3 Proposed Updated FY 2019_2021 MCH Block Grant Gui
Maternal and Child Health Services Block Grant Application/Annual Report Guidance
Part3Proposed Updated FY 2019_2021 MCH Block Grant Guidance Forms. Nov_7_2017
Application/Annual Report with Needs Assessment Summary
OMB: 0915-0172
PART THREE: REPORTING FORMS
Form 1 Application for Federal Assistance (Standard Form - 424)
Form 2 MCH Budget/Expenditure Details
Form 3a Budget and Expenditure Details by Types of Individuals Served (IA and IB)
Form 3b Budget and Expenditure Details by Types of Services (IIA and IIB)
Form 4 Number and Percentage of Newborns and Others Screened, Cases Confirmed and Treated
Form 5a Count of Individuals Served By Title V
Form 5b Total Percentage of Populations Served by Title V
Form 6 Deliveries and Infants Served by Title V and Entitled to Benefits Under Title XIX
Form 7 State MCH Toll-Free Telephone Line and Other Appropriate Methods Data
Form 8 State MCH and CSHCN Directors Contact Information
Form 9 List of MCH Priority Needs
Form 10 Tracking Measures (NPMs, ESMs, SPMs and SOMs)
Form 11 Other State Data (OSD) – #01 - #03

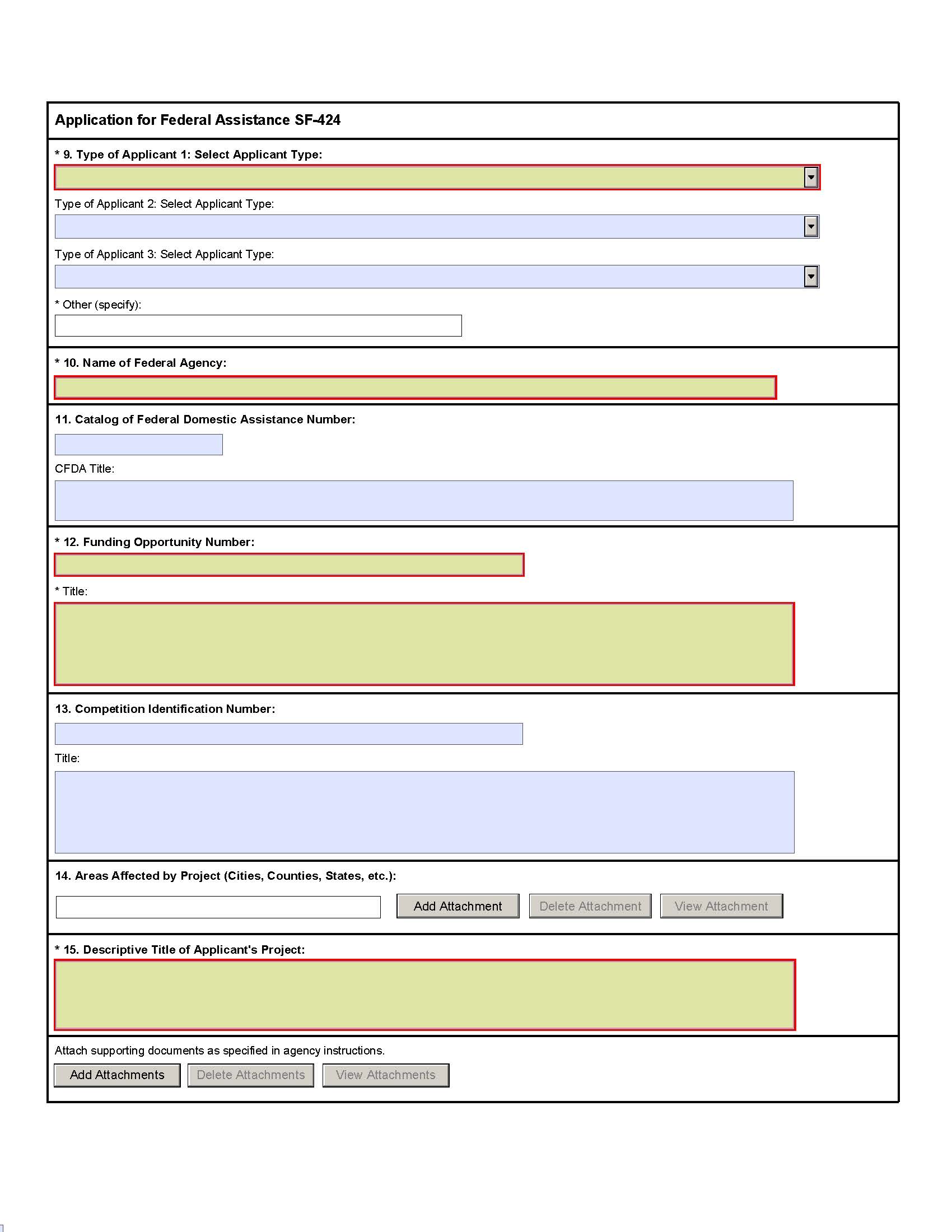
Instructions for Application for Federal Assistance (SF-424)
This is a standard form required for use as a cover sheet for submission of pre-applications and applications and related information under discretionary programs. Some of the items are required and some are optional at the discretion of the applicant or the federal agency (agency). Required fields on the form are identified with an asterisk (*) and are also specified as "Required" in the instructions below. In addition to these instructions, applicants must consult agency instructions to determine other specific requirements.
Item |
Field Name |
Information |
1. |
Type of Submission: |
(Required) Select one type of submission in accordance with agency instructions.
|
2. |
Type of Application: |
(Required) Select one type of application in accordance with agency instructions.
A. Increase
Award |
3. |
Date Received: |
Leave this field blank. This date will be assigned by the Federal agency. |
4. |
Applicant Identifier: |
Enter the entity identifier assigned by the Federal agency, if any, or the applicant's control number if applicable. |
5a. |
Federal Entity Identifier: |
Enter the number assigned to your organization by the federal agency, if any. |
5b. |
Federal Award Identifier: |
For new applications leave blank. For a continuation or revision to an existing award, enter the previously assigned federal award identifier number. If a changed/corrected application, enter the federal identifier in accordance with agency instructions. |
6. |
Date Received by State: |
Leave this field blank. This date will be assigned by the state, if applicable. |
7. |
State Application Identifier: |
Leave this field blank. This identifier will be assigned by the state, if applicable. |
8. |
Applicant Information: |
Enter the following in accordance with agency instructions: |
|
a. Legal Name: |
(Required) Enter the legal name of applicant that will undertake the assistance activity. This is the organization that has registered with the Central Contractor Registry (CCR). Information on registering with CCR may be obtained by visiting www.Grants.gov. |
|
b. Employer/Taxpayer Number (EIN/TIN): |
(Required) Enter the employer or taxpayer identification number (EIN or TIN) as assigned by the Internal Revenue Service. If your organization is not in the US, enter 44-4444444. |
|
c. Organizational DUNS: |
(Required) Enter the organization's DUNS or DUNS+4 number received from Dun and Bradstreet. Information on obtaining a DUNS number may be obtained by visiting www.Grants.gov. |
|
d. Address: |
Enter address: Street 1 (Required); city (Required); County/Parish, State (Required if country is US), Province, Country (Required), 9-digit zip/postal code (Required if country US). |
|
e. Organizational Unit: |
Enter the name of the primary organizational unit, department or division that will undertake the assistance activity. |
|
f. Name and contact information of person to be contacted on matters involving this application: |
Enter the first and last name (Required); prefix, middle name, suffix, title. Enter organizational affiliation if affiliated with an organization other than that in 7.a. Telephone number and email (Required); fax number. |
9. |
Type of Applicant: (Required) Select up to three applicant type(s) in accordance with agency instructions. |
A. State Government |
10. |
Name Of Federal Agency: |
(Required) Enter the name of the federal agency from which assistance is being requested with this application. |
11. |
Catalog Of Federal Domestic Assistance Number/Title: |
Enter the Catalog of Federal Domestic Assistance number and title of the program under which assistance is requested, as found in the program announcement, if applicable. |
12. |
Funding Opportunity Number/Title: |
(Required) Enter the Funding Opportunity Number and title of the opportunity under which assistance is requested, as found in the program announcement. |
13. |
Competition Identification Number/Title: |
Enter the competition identification number and title of the competition under which assistance is requested, if applicable. |
14. |
Areas Affected By Project: |
This data element is intended for use only by programs for which the area(s) affected are likely to be different than the place(s) of performance reported on the SF-424 Project/Performance Site Location(s) Form. Add attachment to enter additional areas, if needed. |
15. |
Descriptive Title of Applicant's Project: |
(Required) Enter a brief descriptive title of the project. If appropriate, attach a map showing project location (e.g., construction or real property projects). For pre-applications, attach a summary description of the project. |
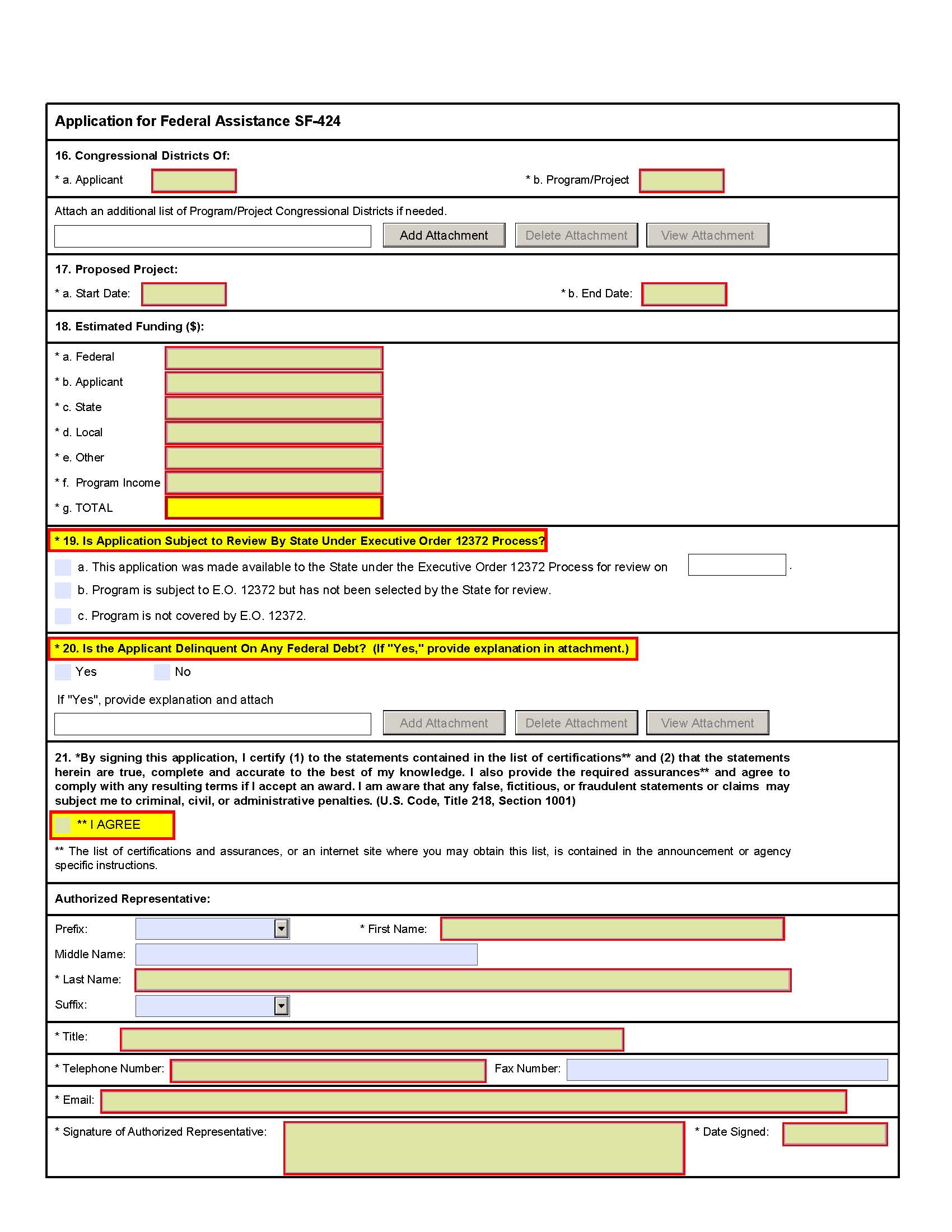
16. |
Congressional Districts Of: |
15a. (Required) Enter the applicant's congressional district. 15b. Enter all district(s) affected by the program or project. Enter in the format: 2 characters state abbreviation - 3 characters district number, e.g., CA-005 for California 5th district, CA-012 for California 12 district, NC-103 for North Carolina's 103 district. If all congressional districts in a state are affected, enter "all" for the district number, e.g., MD-all for all congressional districts in Maryland. If nationwide, i.e. all districts within all states are affected, enter US-all. If the program/project is outside the US, enter 00-000. This optional data element is intended for use only by programs for which the area(s) affected are likely to be different than place(s) of performance reported on the SF-424 Project/Performance Site Location(s) Form. Attach an additional list of program/project congressional districts, if needed. |
17. |
Proposed Project Start and End Dates: |
(Required) Enter the proposed start date and end date of the project. |
18. |
Estimated Funding: |
(Required) Enter the amount requested, or to be contributed during the first funding/budget period by each contributor. Value of in-kind contributions should be included on appropriate lines, as applicable. If the action will result in a dollar change to an existing award, indicate only the amount of the change. For decreases, enclose the amounts in parentheses. |
19. |
Is Application Subject to Review by State Under Executive Order 12372 Process? |
(Required) Applicants should contact the State Single Point of Contact (SPOC) for Federal Executive Order 12372 to determine whether the application is subject to the State intergovernmental review process. Select the appropriate box. If "a." is selected, enter the date the application was submitted to the State. |
20. |
Is the Applicant Delinquent on any Federal Debt? |
(Required) Select the appropriate box. This question applies to the applicant organization, not the person who signs as the authorized representative. Categories of federal debt include; but, may not be limited to: delinquent audit disallowances, loans and taxes. If yes, include an explanation in an attachment. |
21. |
Authorized Representative: |
To be signed and dated by the authorized representative of the applicant organization. Enter the first and last name (Required); prefix, middle name, suffix. Enter title, telephone number, email (Required); and fax number. A copy of the governing body's authorization for you to sign this application as the official representative must be on file in the applicant's office. (Certain federal agencies may require that this authorization be submitted as part of the application.) |
FORM 2
MCH BUDGET/EXPENDITURE DETAILS
[Sections 503(a), 504(d) and 505(a)(3),(4)]

FY__ Application FY__ Annual Report
Budgeted Expended
1. FEDERAL ALLOCATION $___________ $___________
(Referenced items on the Application Face
Sheet [SF-424] apply only to the Application Year)
Of the Federal Allocation, the amount earmarked for:
A. Preventive and Primary Care for Children: $___________ (__%) $___________ (__%)
B. Children with Special Health Care Needs: $___________ (__%) $___________ (__%)
C. Title V Administrative Costs: $___________ (__%) $___________ (__%)
2. SUBTOTAL OF LINES 1A-C (This subtotal does not include)
Pregnant Women and All Others) $___________ $___________
3. STATE MCH FUNDS (Item 18c of SF-424) $___________ $___________
4. LOCAL MCH FUNDS (Item 18d of SF-424) $___________ $___________
5. OTHER FUNDS (Item 18e of the SF-424) $___________ $___________
6. PROGRAM INCOME (Item 18f of SF-424) $___________ $___________
7. TOTAL STATE MATCH (Lines 3 through 6) $___________ $___________
A. Enter your State's FY 1989
Maintenance of Effort Amount $____________________
8. FEDERAL-STATE TITLE V BLOCK GRANT PARTNERSHIP SUBTOTAL $___________ $___________
(Total lines 1 and 7)
9. OTHER FEDERAL FUNDS [Select Appropriate Funding Sources from the Drop-Down Box]
(Report only funds under the control of the Title V Program Administrator)


Select the Appropriate Federal Department

Select the Appropriate Federal Agency.

Select the Appropriate Federal Grant Program.
$___________ $___________
10. OTHER FEDERAL FUNDS (SUBTOTAL of all funds under item 9) $___________ $___________
11. STATE MCH BUDGET/EXPENDITURE GRAND TOTAL
(Partnership Subtotal + Other Federal MCH Funds Subtotal) $__________ $___________
INSTRUCTIONS FOR COMPLETION OF FORM 2
MCH BUDGET/EXPENDITURE DETAILS
Title V Citation: Section 504(d) states: “Of the amounts paid to a State...not more than 10 percent may be used for administering the funds paid....” In order to be entitled to payments for allotments under Title V, Section 505(a)(3) provides that the State will use: “(A) at least 30 percent of such payment amounts for preventive and primary care services for children, and (B) at least 30 percent of such payment amounts for services to children with special health care needs.” Section 505(a)(4) provides that a State receiving funds for maternal and child health services “...shall maintain the level of funds being provided solely by such State for maternal and child health programs at a level at least equal to the level that such State provided for such programs in fiscal year 1989....”
Instructions: This form provides details of the State’s MCH budget and expenditures for the Application year and Annual Report year, respectively, and the fulfillment of certain spending requirements under Title V for a given year. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance. Note: It is recognized that States may not have final expenditure data at the time of submission of the application/annual report. States will report final expenditure data at grant closeout.
Line Number |
Instructions for Application Budgeted |
1 |
The Title V Information System (TVIS) will prepopulate the Federal Title V allocation from the SF 424 (Item 18a). |
|
|
1A |
Enter the amount of the Federal allotment for preventive and primary care for children. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS. |
|
|
1B |
Enter the amount of the Federal allotment for children with special health care needs. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS. |
|
|
1C |
Enter the amount of the Federal allotment for the administration of the allotment. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS. |
|
|
2 |
The TVIS will calculate the subtotal of Lines 1A, 1B and 1C. Please note that Pregnant Women and All Others will not be included in this amount. |
|
|
3 |
The TVIS will prepopulate the amount of your State total funds for the Title V allocation (match) from the SF 424 (Item 18c). |
|
|
4 |
The TVIS will prepopulate the amount of total MCH dedicated matching funds garnered from local jurisdictions within your State from the SF 424 (Item 18d). |
|
|
5 |
The TVIS will prepopulate the total of MCH funds available from other sources such as foundations from the SF 424 (Item 18e). |
|
|
6 |
The TVIS will prepopulate the amount of MCH program income funds collected by your State’s MCH agencies from insurance payments, MEDICAID, HMO’s, etc. from the SF 424 (Item 18f). |
|
|
7 |
The TVIS will calculate the sum total of Lines 3, 4, 5, and 6 for the total of your State match and overmatch. |
|
|
7A |
The TVIS will prepopulate your State’s FY 1989 Maintenance of Effort amount. |
|
|
8 |
The TVIS will calculate the total for Lines 1 and 7. This amount is the “Federal-State Title V Block Grant “Partnership.” |
|
|
9 |
Use the respective drop-down menus in TVIS to select all Federal funding award programs planned to be received by the State MCH program other than the Title V Block Grant that are directly under the control of the Title V Program Administrator and enter planned amounts.
|
|
|
10 |
The TVIS will calculate the sum of all lines in item 9. |
|
|
11 |
The TVIS will calculate the sum of Lines 8 and 10. This amount is the total of all MCH funds administered by your State’s MCH program. |
Line Number |
Instructions for Annual Report Expended |
1
1A
1B
1C
2
3
4
5
6
7
7A
8
9
10
11 |
Enter the Federal Title V allocation received. Note: TVIS will display the original budgeted amounts for reference.
Enter the amount of the Federal allotment for preventive and primary care for children. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS.
Enter the amount of the Federal allotment for children with special health care needs. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS.
Enter the amount of the Federal allotment for the administration of the allotment. The percentage of the total (Line 1) that this amount represents will be calculated by TVIS.
The TVIS will calculate the subtotal of Lines 1A, 1B and 1C. Please note that Pregnant Women and All Others will not be included in this amount.
Enter the amount of your State total funds for the Title V allocation (match).
Enter the amount of total MCH dedicated matching funds garnered from local jurisdictions within your State.
Enter the total of MCH funds available from other sources such as foundations.
Enter the amount of MCH program income funds collected by your State’s MCH agencies from insurance payments, MEDICAID, HMO’s, etc..
The TVIS will calculate the sum total of Lines 3, 4, 5, and 6 for the total of your State match and overmatch.
The TVIS will prepopulate your State’s FY 1989 Maintenance of Effort amount.
The TVIS will calculate the total for Lines 1 and 7. This amount is the “Federal-State Title V Block Grant “Partnership.”
TVIS will prepopulate programs and amounts. Adjust the amounts to reflect actuals expended during the budget period. Use field and form notes for any major changes to awards from what had been projected to be received. For Federal awards budgeted or received that are not included in the menu in TVIS, select “Other” and enter the appropriate information.
The TVIS will calculate the sum of all lines in item 9.
The TVIS will calculate the sum of Lines 8 and 10. This amount is the total of all MCH funds administered by your State’s MCH program.
|
FORM 3a
BUDGET AND EXPENDITURE DETAILS BY TYPES OF INDIVIDUALS SERVED (IA and IB)
[Section 506(a)(2)(A)(iv), Section 505(a)(2)(A-B) and Section 506(a)(1)(A-D)]
I. TYPES OF INDIVIDUALS SERVED
FY ____ Application FY ____ Annual Report
IA. Federal MCH Block Grant |
|
Budgeted |
|
Expended |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
Federal TOTAL
|
|
$_______
|
|
$_______
|
FY ____ Application FY ____ Annual Report
IB. Non-Federal MCH Block Grant |
|
Budgeted |
|
Expended |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
|
|
$_______ |
|
$_______ |
Non-Federal TOTAL
|
|
$_______
|
|
$_______
|
FY ____ Application FY ____ Annual Report
Budgeted Expended

FEDERAL-STATE MCH BLOCK GRANT PARTNERSHIP TOTAL |
|
$_______ |
|
$_______ |
INSTRUCTIONS FOR COMPLETION OF FORM 3a
BUDGET/EXPENDITURE DETAILS BY TYPES OF INDIVIDUALS SERVED
Title V Citation: Section 506(a)(2)(A)(iv) requires that each State submit an annual report of its activities under its Title V program. Among the items required to be reported are, “...the amount spent under this title...by class of individuals served.”
Instructions: Complete all required data cells. If an actual number is not available, the State should provide an estimate. All estimates should be explained in a form or field note. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
Line Number |
Instructions |
I.A.1 – I.A.5 |
Enter the budgeted (Application year) and expended (Annual Report year) amounts for the Federal MCH allocation. Any discrepancies should be addressed with a field or form note in TVIS. **Note: The amounts for Children 1 through 21 years and CSHCN should match the amounts reported on Form 2, Lines 1a and 1b for budgeted (Application year) and expended (Annual Report year), respectively. **Note: Line 2 on Form 2 should not equal 100% if amounts are reported for Pregnant Women. |
|
|
I.A.1 Federal TOTAL |
The TVIS will calculate the sum of the amounts entered for Lines I.A.1 through I.A.5. **Note: The Federal TOTAL should equal the Federal Allocation total minus the Title V Administrative Costs. |
|
|
I.B.1 - I.B.5 |
Enter the budgeted (Application year) and expended (Annual Report year) amounts for the non-Federal Title V program funds. |
|
|
I.B.1 Non-Federal TOTAL |
The TVIS will calculate the sum of the amounts entered for Lines I.B.1 through I.B.5. |
|
|
Federal-State MCH Block Grant Partnership TOTAL |
The TVIS will calculate the sum of the amounts entered for the I.A.1 TOTAL and I.B.1 TOTAL. Use form or field notes to explain any discrepancies or unexpected variations. |
FORM 3b
BUDGET AND EXPENDITURE DETAILS BY TYPES OF SERVICES (IIA and IIB)
[Section 506(a)(2)(A)(iv), Section 505(a)(2)(A-B) and Section 506(a)(1)(A-D)]
II. TYPES OF SERVICES
FY ____ Application FY ____ Annual Report
IIA. Federal MCH Block Grant |
|
Budgeted |
|
Expended |
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
|
|
|
|
|
$_______
|
|
$_______
|
|
|
|
($)_____ ($)_____ ($) _____ ($)_____ ($)_____ ($)_____ ($)_____
|
FY ____ Application FY ____ Annual Report

FEDERAL TOTAL |
|
$_______ |
|
$_______ |
Budgeted Expended
FORM 3b
BUDGET AND EXPENDITURE DETAILS BY TYPES OF SERVICES (IIA and IIB)
[Section 506(a)(2)(A)(iv), Section 505(a)(2)(A-B) and Section 506(a)(1)(A-D)]
II. TYPES OF SERVICES (Continued)
FY ____ Application FY ____ Annual Report
IIB. Non-Federal MCH Block Grant |
|
Budgeted |
|
Expended |
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
|
|
|
|
|
$_______ |
|
$_______ |
|
|
|
|
|
|
|
|
|
|
|
|
$_______
|
|
$_______
|
|
|
|
($) _____ ($) _____ ($) _____ ($) _____ ($) _____ ($) _____ ($) _____
|
FY ____ Application FY ____ Annual Report
NON-FEDERAL TOTAL |
|
$_______ |
|
$_______ |
Budgeted Expended
INSTRUCTIONS FOR THE COMPLETION OF FORM 3b
STATE TITLE V PROGRAM BUDGET AND EXPENDITURES BY TYPES OF SERVICES
Title V Citation: Section 505(a)(2) states, in part, “In order to be entitled to payments for allotments...a State must prepare and transmit to the Secretary an application...that includes for each fiscal year (A) a plan for meeting the needs identified by the statewide needs assessment...and (B) a description of how funds allotted to the State...will be used for the provision and coordination of services to carry out such a plan that shall include - (iii) an identification of the types of services to be provided....”
Section 506(a)(1) states, “Each State shall prepare and submit to the Secretary annual reports on its activities under this title.” Among the items required to be reported (Section 506(a)(2)(A)(i-iv)) are, “...the number of individuals served by the State under this title (by class of individuals), the proportion of each class of such individuals which has health coverage, the types (as defined by the Secretary) of services provided under this title to individuals within each such class, and the amounts spent under this title on each type of services, by class of individuals served.”
Instructions: Complete all required data cells. If an actual number is not available, the State should make an estimate. All estimates should be explained in a form or field note in TVIS. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
Line Number |
Instructions |
II.A.1 |
Of the Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Direct Services. |
|
|
II.A.1.a – II.A.1c |
Of the Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Direct Services by types of services and MCH population group. |
|
|
II.A.2 |
Of the Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Enabling Services. |
|
|
II.A.3 |
Of the Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Public Health Services and Systems. |
|
|
II.A.4 |
Enter the amount of Federal Title V funds expended for services that are closely related to each type of direct service listed. If a service cannot be related to one of the provided choices, the state can choose “Other” and enter the type of service that is supported and amount. |
|
|
Federal TOTAL |
The TVIS will calculate the sum of the Federal amounts entered for Line II.A.1, Line II.A.2 and Line II.A.3. |
INSTRUCTIONS FOR THE COMPLETION OF FORM 3b (Continued)
STATE TITLE V PROGRAM BUDGET AND EXPENDITURES BY TYPES OF SERVICES
Line Number |
Instructions |
II.B.1 |
Of the non-Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Direct Services. |
|
|
II.B.1.a – II.B.1c |
Of the non-Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Direct Services by types of services and MCH population group. |
|
|
II.B.2 |
Of the non-Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Enabling Services. |
|
|
II.B.3 |
Of the non-Federal MCH allocation, enter the Total budgeted (Application year) and expended (Annual Report year) amounts for Public Health Services and Systems. |
|
|
II.B.4 |
Enter the amount of non-Federal Title V funds expended for services that are closely related to each type of direct service listed. If a service cannot be related to one of the provided choices, the state can choose “Other” and enter the type of service that is supported and amount. |
|
|
Non-Federal TOTAL |
The TVIS will calculate the sum of the non-Federal amounts entered for Line II.B.1, Line II.B.2 and Line II.B.3. |
FORM 4
NUMBER AND PERCENTAGE OF NEWBORNS AND OTHERS SCREENED,
CASES CONFIRMED AND TREATED
[Section 506(a)(2)(B)(iii)]

Annual Report Year: _____
Total Births by Occurrence: ____________ Data Source Year: _______
Type of Screening Tests |
(A) Aggregate Total Number Receiving at Least One Screen(1) |
(B) Aggregate Total Number Presumptive Positive Screens |
(C) Aggregate Total Number Confirmed Cases(2) |
(D) Aggregate Total Number Referred for Treatment (3) |
||
No. |
% |
|
|
No. |
% |
|
Select
all applicable screening tests from the core and secondary
conditions in the Recommended Uniform Screening Panel (RUSP)
using the drop down list.
|
|
|
|
|
|
|
Type of Screening Tests |
(A) Total Number Receiving at Least One Screen(1) No. % |
(B) Total Number Presumptive Positive Screens |
(B) Total Number Confirmed Cases(2) |
(B) Total Number Referred for Treatment(3)
No. % |
||
|
No. |
% |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
INSTRUCTIONS FOR THE COMPLETION OF FORM 4
NUMBER AND PERCENTAGE OF NEWBORNS AND OTHERS SCREENED,
CASES CONFIRMED, AND TREATED
Title V Citation: Section 506(a)(1) requires each State to submit an annual report on its activities under Title V. Included in this requirement is the following: (2)(B)(iii) “... information on such other indicators of maternal, infant, and child health care status as the Secretary may specify.”
Instructions: Complete all required data cells for the reporting year. If an actual number is not available, make an estimate. All estimates should be explained in a form or field note in TVIS. A Glossary that contains terms applicable to this Form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
Line Number |
Instructions |
Annual Report Year
Lines: “Total Births by Occurrence” and “Data Source Year” |
TVIS will prepopulate the annual report year.
Enter the total number of occurrent births for the State and the year for which the data apply. Total births by occurrence are to be defined as “all births that occur in the State regardless of residency.” States should use the number submitted by the Vital Records program to the National Center for Health Statistics. The data source year is to be defined as calendar year, January 1 – December 31. Please note that the “Total Births...” figure is related to the “Total infants < 1 year of age” row in Form 5a and 5b, and the “TOTAL INFANTS IN STATE” row in section I of Form 6. While these figures are not expected to match, there should be a fairly close relationship between them. |
|
|
|
All States now screen for at least 29 out of the 34 core conditions on the Recommended Uniform Screening Panel (RUSP). Using the drop down box, select the names of all screening tests specific to your state’s newborn population.
|
|
|
|
Enter additional screening tests specific to your state’s newborn population, such as screenings for other conditions that are not listed in the RUSP. Complete Columns A through D for each of the listed screenings. TVIS will calculate the percentages. |
|
|
|
Enter any screening tests that are specific to older children and women. Complete Columns A through D for each of the listed screenings. Note that the % (percentage) portion of Column A is not to be completed since the denominator of Total Births by Occurrence does not apply. Enter the specific names of any other screens that are not listed and complete Columns A through D. |
FORM 5a
COUNT OF INDIVIDUALS SERVED BY TITLE V
(By Class of Individuals and Percent of Health Coverage)
[Section 506(a)(2)(A)(i-ii)]

Annual Report Year__________ |
(A) |
(B) |
(C) |
(D) |
(E) |
(F) |
Type of Individuals Served |
TITLE V |
PRIMARY SOURCE OF COVERAGE |
||||
Total Served |
Title XIX |
Title XXI |
Private/Other |
None |
Unknown |
|
% |
% |
% |
% |
% |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Children with Special Health Care Needs |
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
FORM 5b
TOTAL PERCENTAGE OF POPULATIONS SERVED BY TITLE V
(By Class of Individuals)
[Section 506(a)(2)(A)(i-ii)]
Annual Report Year ________ |
|
Population Served by Title V |
Total % Served |
|
_______ |
|
_______ |
|
_______ |
|
_______ |
|
_______ |
INSTRUCTIONS FOR THE COMPLETION OF FORM 5a and FORM 5b
COUNT OF INDIVIDUALS SERVED BY TITLE V
AND
TOTAL PERCENTAGE OF POPULATIONS SERVED BY TITLE V
[Section 506(a)(2)(A)(i-ii)]
Title V Citation: Section 506(a)(1) requires each State to submit an annual report on its activities under Title V. Included in this requirement is the following: “(2) Each annual report...shall include the following information: (A)(i) The number of individuals served by the State under the title (by class of individuals)…(ii) The proportion of each class of such individuals which has health coverage.”
Instructions: Complete all required data cells for the reporting year. If an actual number is not available, the State should make an estimate. In particular, Form 5b and the insurance coverage section in Form 5a may require estimation. All methods, data sources and included services/programs should be explained in field notes in TVIS. A Glossary that contains terms applicable to this form and examples of included services/programs in each participant category is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
The purpose of Form 5a and Form 5b is two-fold.
Form 5a, Count of Individuals Served by Title V, enables the State to track and report on the number who received an individually-delivered service funded by the Title V program without full reimbursement within the top two levels of the MCH Pyramid (direct and enabling services).
Form 5b, Total Percentage of Population Served by Title V, enables the State to track and report on the total percentage who received a Title V-supported service within all levels of the MCH Pyramid (direct services, enabling services, and public health services and systems).
Since States began to report Title V program participant data in the 1990’s, MCH programs have seen a shift in the delivery of services from direct primary care MCH services to public health and preventive services within well-coordinated and comprehensive systems of care that are designed for the MCH population. This shift has resulted in a need for more complete reporting of individuals served by Title V, which goes beyond an unduplicated count of individuals served (often derived from reimbursement data or individual client records for MCH direct and enabling services).
It is recognized that precisely quantifying the number of individuals reached through the administration or promotion of population-based services and systems (e.g., injury prevention and education, regionalized systems of perinatal care, newborn screening programs) is difficult, and informed estimates are often required. Relying only on reimbursement data or individual client program records supported by Title V, however, can lead to serious underestimates of the number of individuals in a State who actually received and benefitted from a Title V-supported service. For this reason, Form 5b was developed to better capture the full “reach” of the State’s Title V program in serving its MCH population.
Unlike Forms 3a and 3b, the totals reported on Forms 5a and 5b reflect both Federal and Non-federal Title V program dollars.
INSTRUCTIONS FOR THE COMPLETION OF FORM 5a and FORM 5b
COUNT OF INDIVIDUALS SERVED BY TITLE V
AND
TOTAL PERCENTAGE OF POPULATIONS SERVED BY TITLE V
[Section 506(a)(2)(A)(i-ii)]
Form/Line Number |
Instructions |
Form 5a |
States should report the number of individuals who received a direct or enabling service funded by Title V in each of the listed MCH population groups, along with the percentage of each group by insurance coverage type. |
|
|
Report Year |
TVIS will prepopulate the annual report year for which the data apply. |
|
|
1 – 5, Column A |
Enter the best possible estimate for the number who received an individually-delivered direct or enabling service funded by the Title V program without full reimbursement. This number includes individuals who received a service funded by total Federal and Non-federal dollars as reported on line 8 of Form 2, and it should align with the combined totals on Form 3a and 3b for direct and enabling services. Pregnant women may also receive non-pregnancy related services and be counted in other participant categories (i.e., Children ages 1 through 21 and Others). All remaining categories are mutually exclusive, with CSHCN reported as a subset of all children ages 1 through 21. Within each reporting category, the count of individuals served should be unduplicated to the fullest extent possible. All methods, data sources, and included services/programs should be explained in field notes in TVIS. |
|
|
1 -5, Columns B - F |
Enter the percentages of individuals reported in Column A by their primary source of coverage. If insurance status is unknown, states should report an estimate. Estimates from population-based data sources will be provided by MCHB to facilitate reporting. |
|
|
Form 5b |
States should report an estimate for the total percentage of populations who received a Title V-supported service in each of the listed MCH population groups across all levels of the MCH Pyramid, including public health services and systems. |
|
|
Report Year |
TVIS will prepopulate the annual report year for which the data apply. |
|
|
1-5 |
Enter the best possible estimate for a total percentage of each population group served by the Title V program across all levels of the MCH Pyramid (i.e. direct services, enabling services, and public health services and systems). This estimate includes all individuals and populations served by the total Federal and State dollars as reported on line 8 of Form 2 and the combined totals on Form 3a and 3b for all service levels. Non-Title V programs that provide direct and enabling services (e.g., WIC, Home Visiting) may be included if Title V funds or staff time are used to promote or enhance services (individual services that are Title V funded may also be counted in 5a). To avoid duplication, numerators for the percentage estimate should focus on the programs and services that have the largest reach for a given population, which generally involves public health services and systems. Approximate denominators for each population group will be provided by MCHB to facilitate percentage estimation. Within public health services and systems, only those populations who are reached by activities that directly promote access or quality of specific population-based services and systems should be counted (see examples in Appendix H of the Supporting Documents). All methods, data sources, and included services/programs should be explained in field notes in TVIS.
|
FORM 6
DELIVERIES AND INFANTS SERVED BY TITLE V
AND ENTITLED TO BENEFITS UNDER TITLE XIX
(By Race and Ethnicity)
[Section 506(a)(2)(C-D)]

UNDUPLICATED COUNT BY RACE/ETHNICITY
Annual Report Year: ________
|
(A) TOTAL |
(B) Non-HispanicWhite |
(C) Non-Hispanic Black or African American |
(D) Hispanic |
(E) Non-Hispanic American Indian or Native Alaskan |
(F)
Non-Hispanic
Asian
|
(G) Non-Hispanic Native Hawaiian or Other Pacific Islander |
(H) Non-Hispanic Multiple Race |
(I) Other & Un-known |
IN STATE |
|
|
|
|
|
|
|
|
|
TITLE V SERVED |
|
|
|
|
|
|
|
|
|
ELIGIBLE FOR TITLE XIX |
|
|
|
|
|
|
|
|
|
IN STATE |
|
|
|
|
|
|
|
|
|
TITLE V SERVED |
|
|
|
|
|
|
|
|
|
ELIGIBLE FOR TITLE XIX |
|
|
|
|
|
|
|
|
|
INSTRUCTIONS FOR THE COMPLETION OF FORM 6
DELIVERIES AND INFANTS SERVED BY TITLE V
AND ENTITLED TO BENEFITS UNDER TITLE XIX
Title V Citation: Section 506 (a)(1) requires each State to submit an Annual Report on its activities under Title V. Included in this requirement is the following:
(2)(C) “Information (by racial and ethnic group) on--
(i) the number of deliveries in the State in the year, and
(ii) the number of such deliveries to pregnant women who were provided prenatal, delivery, or postpartum care under this title or were entitled to benefits with respect to such deliveries under the State plan under title XIX in the year.
(2)(D) Information (by racial and ethnic group) on--
(i) the number of infants under one year of age who were in the State in the year, and
(ii) the number of such infants who were provided services under this title or were entitled to benefits under the State plan under title XIX at any time during the year.”
Instructions: Complete all required data cells for the annual report year. If an actual number is not available, the State should make an estimate. All estimates should be explained in a form or field note in TVIS. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance. It is recognized that there will be overlap between the reported totals for “Title V Served” and “Eligible for Title XIX”, due to an individual’s changing insurance eligibility status during the course of a year (i.e., “churning”.) Form 6 asks for all individuals who are served by Title V and an estimate of the individuals in the State who are eligible for Title XIX. The form does not ask for a report on those individuals served by Title V who are also eligible for Title XIX.
Line Number |
Instructions |
Section I: Unduplicated Count by Race/Ethnicity |
|
Annual Report Year
Total Deliveries in State |
TVIS will prepopulate the annual report year for which the data apply.
In columns A, enter the number for the population-based total of all deliveries in the State for the reporting year eligible for Title XIX who were provided delivery of services in the reporting year. For Columns B-I, enter the number of individuals who were eligible by race and ethnicity. TVIS will calculate the total in columns A based on the numbers provided by race/ethnicity. |
|
|
Total Infants in State |
In column A, enter the number of infants, which is related to the “Total Births by Occurrence” line in Form 4. The “Total Infants <1 year of age” served by Title V is related to the count of infants served in Form 5b. While these figures may not match exactly, they should show a fairly close relationship to each other. For columns B-I, enter the number of infants who were eligible by race and ethnicity. TVIS will calculate the total in columns A based on the numbers provided by race/ethnicity. |
FORM 7
STATE MCH TOLL-FREE TELEPHONE LINE AND OTHER APPROPRIATE METHODS DATA
State MCH Toll-Free Telephone Line [Sections 505(a)(5)(E) and 509(a)(8)]:
STATE: _______
|
Application Year__ Annual Report Year__ |
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
Other Appropriate Methods [Sections 505(a)(5)(E) and 509(a)(8)]:
|
Application Year__ Annual Report Year__ |
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
|
________________________________________ |
|
|
INSTRUCTIONS FOR THE COMPLETION OF FORM 7
STATE MCH TOLL-FREE TELEPHONE LINE AND OTHER APPROPRIATE METHODS DATA
Title V Citation: Section 505(a)(5)(E) states, in part, “the State agency (or agencies) administering the State’s program under this title will provide for a toll-free telephone number (and other appropriate methods) for the use of parents to access information about health care providers and practitioners who provide health care services under this title and title XIX and about other relevant health and health-related providers and practitioners...”
The Maternal and Child Health Bureau is the designee of the Secretary of the Department of Health and Human Services to carry out the mandate of Section 509(a)(8) of Title V, which requires that a national directory of toll-free numbers be made available to State agencies that administer the State’s Title V programs.
Instructions: Complete all required data cells for the application and annual report year, as specified. If an actual total number of calls received or total hits to the website is not available, the State should make an estimate. All estimates should be explained in a form or field note in TVIS.
Line Number |
Instructions |
State |
TVIS will prepopulate the name of the State. |
|
|
Year |
|
|
|
A.1 |
Enter the State’s primary toll-free MCH information line telephone number. |
|
|
A.2 |
Enter the name of the State’s primary toll-free MCH information line. |
|
|
A.3 |
Enter the name of the person who should be contacted with any concerns about the State’s primary toll-free MCH information line. |
|
|
A.4 |
Enter the telephone number of the contact person that is listed on Line A.3. |
|
|
A.5 |
For the annual report year only, enter the number of calls received on the State’s primary toll-free MCH information line. |
|
|
Line Number |
Instructions |
B.1 |
Enter the names of other toll-free information lines that are administered by the State. |
|
|
B.2 |
For the annual report year, enter the number of calls received by the other toll-free MCH information lines administered by the State. |
|
|
B.3 |
Enter the URL for the State Title V Program website. |
|
|
B.4 |
For the annual report year only, enter the number of hits to the State Title V Program website address listed on Line B.3. |
|
|
B.5 |
Enter the URLs for the State Title V Social Media Websites |
|
|
B.6 |
For the annual report year only, enter the number of hits to the State Title V Program social media website addresses listed on Line B.5. |
|
|
FORM 8
STATE MCH AND CSHCN DIRECTORS CONTACT INFORMATION
FOR APPLICATION YEAR____
STATE: __________________________
|
|
Name: |
__________________________________ |
Title |
__________________________________ |
Street Address: |
__________________________________ |
Room Number: |
__________________________________ |
City/State/Zip: |
__________________________________ |
Telephone: |
__________________________________ |
Email: |
__________________________________ |
|
|
|
|
Name: |
__________________________________ |
Title |
__________________________________ |
Street Address: |
__________________________________ |
Room Number: |
__________________________________ |
City/State/Zip: |
__________________________________ |
Telephone: |
__________________________________ |
Email: |
__________________________________ |
|
|
|
|
Name: |
__________________________________ |
Title |
__________________________________ |
Street Address: |
__________________________________ |
Room Number: |
__________________________________ |
City/State/Zip: |
__________________________________ |
Telephone: |
__________________________________ |
Email: |
__________________________________ |
|
|
Instructions: TVIS will prepopulate the name of the State and the application year. Enter the name of the Title V MCH Director, CSHCN Director and, at the option of the State, the Family and/or Youth Leader. For each of the listed contacts, provide the title, address, telephone number and e-mail address.
FORM 9
LIST OF MCH PRIORITY NEEDS
[Section 505(a)(1)]
Your state’s Five-Year Statewide Needs Assessment should identify the need for preventive and primary care services for pregnant women, mothers, and infants; preventive and primary care services for children; and services for Children with Special Health Care Needs. The established priorities should guide the activities that are included in the State's Five-year Action Plan. In order to evaluate success in meeting the goals of the priority needs, the State should determine, at the time of priority setting, its plan for assessing if priority needs have been addressed. This assessment should include the development of State Performance Measures (SPMs), which are specifically tailored to a priority need to the extent that such need is not fully addressed by the National Performance Measures (NPMs) or the State Evidence-based or –informed Strategy Measures (ESMs).
Instructions: With each year’s Block Grant Application, the State should provide a list, (whether or not the priority needs change) of its top maternal and child health needs and crosslink the identified priorities with the existing National Outcome Measures (NOMs), NPMs, SPMs and ESMs. Use a simple sentence or phrase to list your State’s needs below. Examples of such statements are: “To reduce the barriers to the delivery of care for pregnant women,” and “The infant mortality rate for minorities should be reduced.” For each priority, indicate if it a new priority need for this five-year reporting cycle or if it is being revised or continued from the previous five-year cycle. Please note that TVIS will prepopulate the priority needs provided in the previous year.
MCHB will capture annually every State’s top 7 to 10 priority needs in TVIS for comparison, tracking, and reporting purposes. The State must list at least 7 priority needs, and the form will only accept up to 10. If desired, the State may list and describe additional priority needs in a form note. Note that the numerical listing below is for computer tracking only and is not meant to indicate a priority order.
STATE__________________________________ APPLICATION YEAR______
-
PRIORITY NEEDS
NEW (N), REVISED (R) OR CONTINUED (C) PRIORITY NEED FOR THIS FIVE-YEAR REPORTING PERIOD
N
R
C
1
2
3
4
5
6
7
8
9
10
FORM 10
TRACKING MEASURES
National Performance Measures (NPMs), Evidence-based or –Informed Strategy Measures (ESMs), State Performance Measures (SPMs) and State Outcome Measures (SOMs)
[Sections 505(a)(2)(B)(i),(iii) and 506(a)(2)(A)(iii)]

10a. NPM Annual Report Year: Objective and Performance Data
Click here to view Federally Available Data ⃝ Click here to view MCHB provided Detail Sheet ⃝
MEASURE #__ (Measure Title) |
Annual Report Year: |
FY__ |
FY__
|
FY__ |
FY__ |
FY__ |
|
Annual Objective |
______ |
______ |
______ |
______ |
______ |
______ |
|
Annual Indicator |
______ |
|
|
|
|
|
|
Numerator |
______ |
|
|
|
|
|
|
Denominator |
______ |
|
|
|
|
|
|
Data Source: ________ Data Source Year: _____ |
|
|
|
|
|
||
Provisional or Final?: ⃝ Provisional ⃝ Final |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Click here to provide note: ⃝
10b. ESM Annual Report Year: Objective and Performance Data
Click here to create/view Detail Sheet (10e) ⃝
MEASURE #__ (Measure Title) |
Annual Report Year: |
FY__ |
FY__
|
FY__ |
FY__ |
FY__ |
|
Annual Objective |
______ |
______ |
______ |
______ |
______ |
______ |
|
Annual Indicator |
______ |
|
|
|
|
|
|
Numerator |
______ |
|
|
|
|
|
|
Denominator |
______ |
|
|
|
|
|
|
Data Source: ________ Data Source Year: _____ |
|
|
|
|
|
||
Provisional or Final?: ⃝ Provisional ⃝ Final |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Click here to provide note: ⃝
10c. SPM Annual Report Year: Objective and Performance Data
Click here create/view Detail Sheet (10e) ⃝
MEASURE #__ (Measure Title) |
Annual Report Year: |
FY__ |
FY__
|
FY__ |
FY__ |
FY__ |
|
Annual Objective |
______ |
______ |
______ |
______ |
______ |
______ |
|
Annual Indicator |
______ |
|
|
|
|
|
|
Numerator |
______ |
|
|
|
|
|
|
Denominator |
______ |
|
|
|
|
|
|
Data Source: ________ Data Source Year: _____ |
|
|
|
|
|
||
Provisional or Final?: ⃝ Provisional ⃝ Final |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Click here to provide note: ⃝
10d. SOM Annual Report Year: Objective and Performance Data (Optional)
Click here for Detail Sheet (10e) ⃝
MEASURE #__ (Measure Title) |
Annual Report Year: |
FY__ |
FY__
|
FY__ |
FY__ |
FY__ |
|
Annual Objective |
______ |
______ |
______ |
______ |
______ |
______ |
|
Annual Indicator |
______ |
|
|
|
|
|
|
Numerator |
______ |
|
|
|
|
|
|
Denominator |
______ |
|
|
|
|
|
|
Data Source: ________ Data Source Year: _____ |
|
|
|
|
|
||
Provisional or Final?: ⃝ Provisional ⃝ Final |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Click here to provide note: ⃝
10e. ESM/SPM/SOM Detail Sheet
ESM/SPM/SOM # ___________
PERFORMANCE MEASURE TITLE: |
|
|
|
For SPMs and SOMs only: CHOOSE THE POPULATION DOMAIN(S) TO WHICH THIS MEASURE RELATES: |

Select the Domain(s)
|
For ESMs Only: CHOOSE THE NPM TO WHICH THIS ESM IS LINKED: (Choose one)
CHOOSE THE ESM SUBGROUP (IF RELEVANT): (Choose one or more)
|


Select Subgroup (if
relevant)
Select the National
Performance Measure
|
GOAL
|
|
DEFINITION
|
Numerator: Denominator: Units: ________ _________ (Number) (Text)
|
HEALTHY PEOPLE 2020 OBJECTIVE
|
|
DATA SOURCES and DATA ISSUES
|
|
SIGNIFICANCE
|
|
INSTRUCTIONS FOR THE COMPLETION OF FORM 10
TRACKING MEASURES
National Performance Measures (NPMs), Evidence-based or –Informed Strategy Measures (ESMs), State Performance Measures (SPMs) and State Outcome Measures (SOMs)
Title V Citation: Section 505(a)(2)(B)(i),(iii) requires the States to submit an Application that includes, ...a statement of the goals and objectives consistent with the health status goals and national health objectives...for meeting the needs specified in the State plan...[and]...an identification of the types of services to be provided... “Section 506(a)(2)(A)(iii) requires the States to report annually on the ...type (as defined by the Secretary) of services provided under this title...”
Instructions: As the standard form to be used by States in tracking all measurement types (e.g., NOMs, NPMs, ESMs, SPMs and SOMs) specified in this Guidance, this form serves a dual purpose: 1) Displays 5-year planned objectives (targets) for each NPM, ESM, SPM and SOM, as applicable, as part of the Application, and 2) Reports Annual Indicators, values actually achieved during a reporting year, for each NPM, SPM, ESM and SOM, as applicable, as part of the Annual Report. States are not required to establish performance targets for the NOMs. For the NPMs and the NOMs, the Annual Indicator data will be populated annually by the Maternal and Child Health Bureau, as available, using the referenced national data source identified on the detail sheet for each specific NPM and NOM. While not responsible for entering an Annual Indicator, States will be responsible for tracking their annual progress on the NPMs and their related NOMs. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
For the Application Year, States will establish five-year performance targets for each selected NPM, ESM, SPM and SOM, as applicable. Within the five-year period, performance targets that were established by the State in previous years’ Applications will be pre-populated on the form.
For the annual report year, TVIS will prepopulate the federally available indicator data for the NOMs and the NPMs. If federal indicator data is not available for a measure chosen by the state, the state will be required to provide state data for their five chosen NPMs. States will complete the required data cells (i.e., Annual Indicator, Numerator, Denominator, Data Source and Reporting Note) for the ESMs, SPMs and SOMs, if applicable. If the final data are not available, the State should provide provisional or estimated data with an explanation in a field note in TVIS.
Line Number |
Instructions FOR 10a-10d |
Measure Number
|
The TVIS will prepopulate the measure number. |
Annual Report Year
|
The TVIS will prepopulate the annual report years. |
Annual Objective
|
Enter the Annual Objective (for the most recently added out-year). The TVIS will prepopulate objectives provided in previous years.
|
Annual Indicator |
For the current annual report year, enter the Annual Indicator, including the Numerator and Denominator, for each ESM, SPM and SOM. The TVIS will prepopulate the Annual Indicator from federal sources, where available for the NPMs. If federal data is not available, enter the Annual Indicator, including the Numerator and Denominator for the five chosen NPMs. |
|
|
Data Source
|
For the current annual report year, enter the Data Source for the reported Annual Indicator for each ESM, SPM and SOM. The TVIS will prepopulate the Data Source from federal sources, where available for the NPMs. If federal data is not available, enter the Data Source for the five chosen NPMs.
|
Data Source Year
|
For the current annual reporting year, enter the Data Source Year for the reported Annual Indicator for each ESM, SPM and SOM. The TVIS will prepopulate the Data Source Year from federal sources, where available for the NPMs. If federal data is not available, enter the Data Source Year for the five chosen NPMs.
|
Provisional/Final?
|
Check the button in TVIS to indicate if the data is provisional or final. |
Note |
For the current annual reporting year, enter a data note to clarify any estimated or provisional data and to describe other limitations which impact the reporting of an Annual Indicator for each NPM, ESM, SPM and SOM. |
Instructions: Section 10e of this form is used for creating an ESM, SPM or SOM. Complete each section as appropriate for the measure being described. Note that the measure title and numerator and denominator data will be displayed in TVIS on the respective section (e.g., 10b, 10c and 10d) as they are defined on this form. A Glossary that contains terms applicable to this form is provided in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
Line Number |
Instructions for 10e |
ESM, SPM or SOM # |
TVIS will prepopulate the measure number.
|
Performance Measure Title
|
Enter a brief, narrative description of the performance or outcome measure. |
Choose the Population Domain(s) to which this SPM or SOM is linked
Choose the NPM to which this ESM is linked
Choose ESM Subgroup (if relevant)
|
Select the related population domain(s) from the displayed pick list, as applicable.
Select the related national performance measure from the displayed pick list in TVIS.
If focusing on a subpopulation group, select the subgroup from the displayed pick list in TVIS. Refer to Table 1 in Appendix E for a list of subgroups.
|
Goal
Definition
Healthy People 2020 Objective
Data Source & Data Issues
Significance |
Enter a short statement indicating what the State hopes to accomplish by tracking this measure. Numerator: If the measure is a percentage, rate, or ratio, provide a clear description of the numerator. Denominator: If the measure is a percentage, rate, or ratio, provide a clear description of the denominator. Units: If the measure is a percentage, rate, ratio, or scale, indicate the units in which the measure is to be expressed (e.g., 10,000; 1,000; 100) by selecting a choice in pick list for the "Number" field. Select the type of measure from the pick list (e.g., percentage, rate, ratio, scale, yes/no) on "Text" field.
If the measure is related to a Healthy People 2020 objective describe the objective and corresponding number.
Enter the source(s) of the data used in determining the value of the measure and any issues concerning the methods of data collection or limitations of the data used.
Briefly describe why this measure is significant, especially as it relates to the Goal. Describe also how the value of the measure is determined from the data. If the value of the measure is a scale or a “yes/no,” a clear description of what those values mean and how they are determined should be provided. |
|
|
FORM 11
OTHER STATE DATA (OSD) – #01- #03
(Prepopulated by MCHB, as available)

OSD #01 – Rates of infant mortality, low birth weight, and preterm birth by race and ethnicity
[Section 506 (a)(2)(B)(i)]
Annual Report Year _________
CATEGORY RATE BY RACE/ETHNICITY |
STATE RATE |
NON-HISPANIC WHITE |
NON-HISPANIC BLACK OR AFRICAN AMERICAN |
HISPANIC |
NON-HISPANIC AMERICAN INDIAN OR NATIVE ALASKAN |
NON-HISPANIC ASIAN |
NON-HISPANIC NATIVE HAWAIIAN OR OTHER PACIFIC ISLANDER |
NON-HISPANIC MULTIPLE RACE |
Infant Mortality (Rate per 1,000) |
|
|
|
|
|
|
|
|
Low Birth Weight (%) |
|
|
|
|
|
|
|
|
Preterm Birth (%) |
|
|
|
|
|
|
|
|
OSD #02 – Rates of infant mortality, low birth weight, and preterm birth by county
[Section 506 (a)(2)(B)(i)]
COUNTY (List each County) |
INFANT MORTALITY (Rate per 1,000) |
LOW BIRTH WEIGHT (%) |
PRETERM BIRTH (%) |
|
|
|
|
OSD #03 –State MCH Workforce
[Section 506 (a)(2)(E)(i-vi)]
WORKFORCE CATEGORY |
TOTAL NUMBER |
OBSTETRICIANS |
|
FAMILY PRACTITIONERS |
|
CERTIFIED FAMILY NURSE PRACTITIONERS |
|
CERTIFIED NURSE MIDWIVES |
|
PEDIATRICIANS |
|
CERTIFIED PEDIATRIC NURSE PRACTITIONERS |
|
INSTRUCTIONS FOR THE COMPLETION OF
FORM 11
OTHER STATE DATA (OSD) – #01 - #03
Title V Citation: See OSD reporting tables above.
Instructions: A glossary of terms applicable to this form is presented in Appendix H of the Supporting Documents, which accompany the Application/Annual Report Guidance.
States are not required to collect or report on any of the OSD elements. The purpose of this form is to make available, annually, other State data required by the Title V legislation. Required data elements on this form will be provided by the Maternal and Child Health Bureau (MCHB) in TVIS, as available, for the States. States should review and monitor the annual data.
The racial and ethnic population categories included in these tables are based on the Office of Management and Budget guidelines. More specific instructions are provided below.
TVIS will provide the year for which the data are being reported.
Form Number |
Instructions |
OSD #01: |
In the column labeled “STATE RATE,” the rate for the State is provided in TVIS in the category specified. In the next seven columns the rate of the State in the racial/ethnic categories indicated at the head of each column and in the categories specified is provided in TVIS. Since these data are reported by rates, these data are not totaled. |
|
|
OSD #02 |
Data are provided in TVIS for the rate of infant mortality, low birth weight, and preterm birth by each county in the State. In the first column of the first row, the name of the county is provided. In the second cell of the first row, the rate of infant mortality for that county is provided. In the third cell of the first row, the rate of low birth weight for that county is provided. In the fourth cell of the first row, the rate of preterm birth is provided. In subsequent rows, the names of each county and the rates requested are provided. Depending on the size of the population being reported for each county, rates may use a three-year moving average. Since these data are reported by rates, these data are not totaled. |
|
|
OSD #03 |
Data are provided in TVIS for the numbers of MCH workforce professionals noted that are licensed in the State in the reporting year identified. In the second cell of the first row, the number of obstetricians is provided. In the second cell of the each remaining rows, the number of family practitioners, certified family nurse practitioners, certified nurse midwives, pediatricians, and certified pediatric nurse practitioners are provided, as noted. |
|
|
1 TVIS will use occurrent births as denominator.
2 Report only those from resident births.
3 TVIS will use number of confirmed cases as denominator.
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Author | mlawler |
| File Modified | 0000-00-00 |
| File Created | 2021-01-21 |
© 2025 OMB.report | Privacy Policy