Form 3 Appendix 1C Smoking Cessation Questions
Collection of Customer Service, Demographic and Smoking/Tobacco Use Information from NCI's Contact Center, Cancer Information Service (CIS) Clients
Appendix 1C Smoking Cessation Questions SCIF
Smoking Cessation Clients Smoking Cessation "Intake" Questions
OMB: 0925-0208
NCI/Office of Communications and Public Liaison |
APPENDIX 1C |
SMOKING CESSATION INTAKE QUESTIONS AND DEMOGRAPHIC QUESTIONS (SCIF) |
|
 Demographic
Questions
Demographic
Questions
Smoking Cessation Intake Questions
Dependency – Symptoms
Dependency – Triggers
Dependency – Past Meds

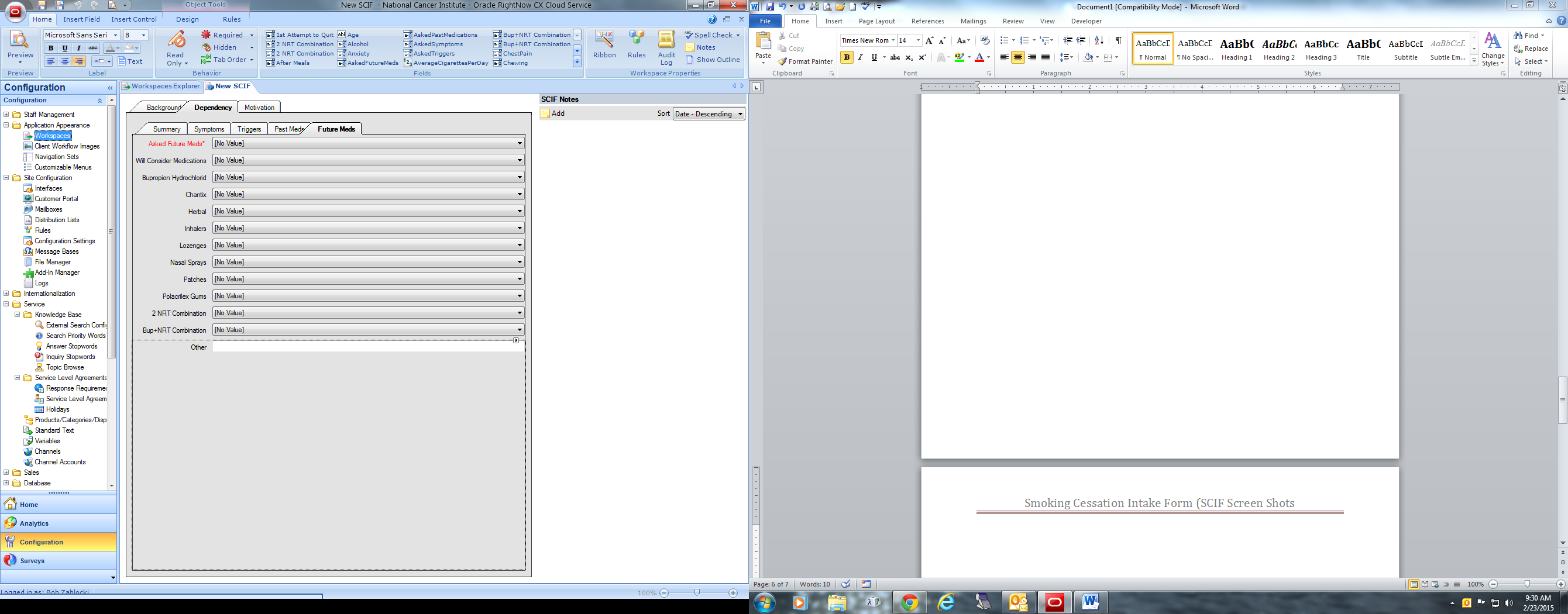
Dependency – Future Meds
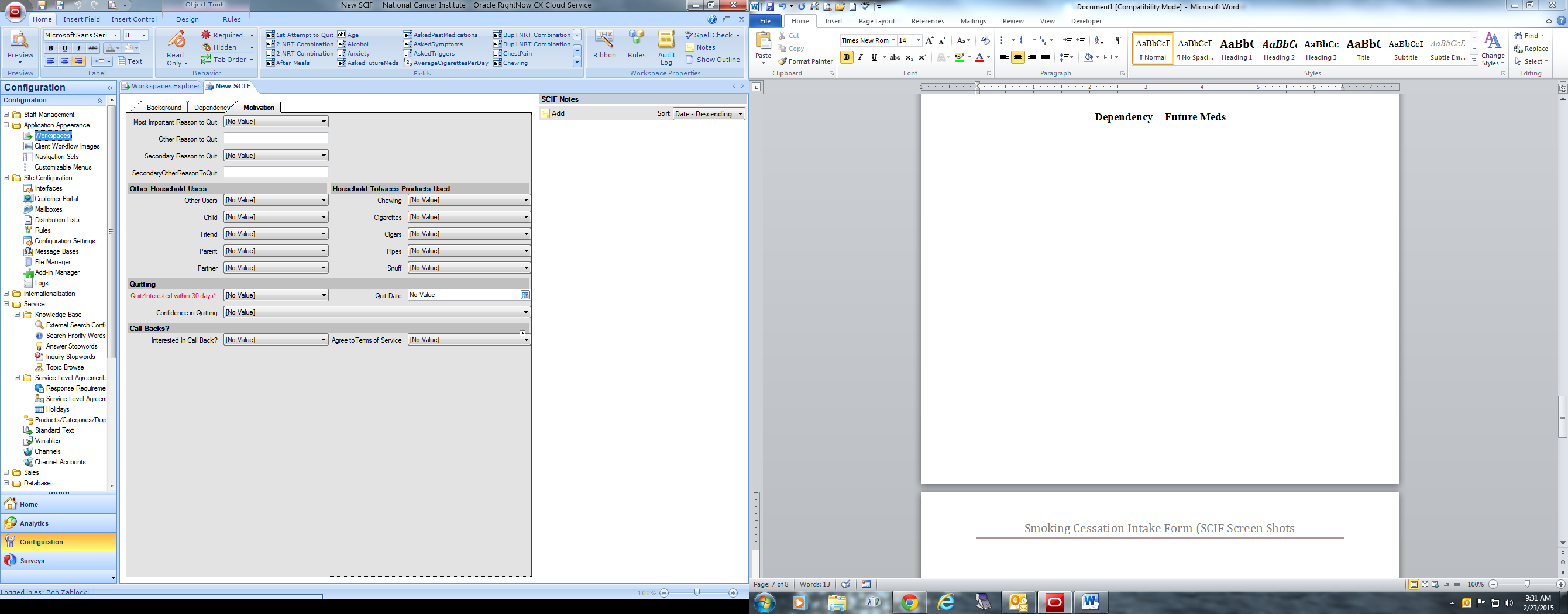
Motivation
Service
Subject of Interaction
Subject 1
No Value
Hospital/Clinic/Physician/Second Opinion
General Cancer Site Information
Treatment/Side Effects
Hospice/Palliative Care/Home Care/Supplies
Financial Assistance
Monetary/Personal Property Donations
Publication Request
Other Inquiry
Screening Mammogram
Diagnostic Mammogram
Pap Test
PSA Test
Screening Colonoscopy
Screening Spiral CT for Lung
Screening MRI for Breast
Diagnostic MRI for Breast
Other Diagnostic Test
Other Screening Test
CT-General Information Only
CT-General Information and Search
CT-CCR Clinical Trials
CT-Results and Outcomes
Support Groups/Counseling Services
Emotional Wellness
Other Psychosocial Issue
Suicidal Client
HPV
Heredity/Genetics/Family History
Environmental Risk Factors
Diet and Nutrition for Prevention
Exercise/Obesity for Prevention/Risk
Hormone Use and Cancer Risk
HIV/AIDS
EMF – Cell Phones
EMF – Other
Other Risk Factors
CAM General Information
CAM – Biologically Based Products
CAM-Mind Body/Spirituality/Energy Med
CAM-Manual Therapies
CAM-Whole Systems
Medical Marijuana
Body/Tissue/Hair Donations
Genetic Services
Report/Statistics
Proton Beam Radiation (txt/side effects)
NCI Programs & Initiatives
Employment at NCI
NCI Budget
NCI Funding Opportunities
Scientific Materials for Researchers
NCI & ARRA
Cancer.gov Comments or Questions
Problems with CT Search
NCI Logo Request
Artwork Request
NCI Other
Cigarettes
Cigars, Cigarillos or Little Cigars
Pipes
Chewing Tobacco, Snuff, or Dip
Other Tobacco
Secondhand Smoke
Marijuana (recreational use)
Cessation Counseling/Information
Subject 2 Same as 1
Subject 3 Same as 1
Subject 4 Same as 1
Subject 5 Same as 1
Cancer Site 1
Aids-related cancers
ALL
AML
Anal
Biliary tract
Bladder
Brain
Breast
Carcinoma of unknown primary
Cervical
CLL
CML
Colorectal
Endometrial/Uterine
Esophageal
Eye
Gastrointestinal carcinoid tumor/GIST
Head and neck
Hodgkin lymphoma
Myeloma/Plasma cell neoplasm
Non-Hodgkin lymphoma
Ovarian
Pancreas
Prostate
Renal (kidney) and renal pelvis
Skin cancer (nonmelanoma)
Small intestine
Soft tissue
Stomach/Gastric
Thyroid
Break off
Other – Central nervous system
Other – Digestive
Other – Endocrine system
Other – Hematologic system
Other – Leukemia
Other – Lymphoma
Other – Musculoskeletal and connective tissue
Other – Reproductive, female
Other – Reproductive, mal
Other – Respiratory
Other – Urinary organs
Other cancers
Childhood cancers
Not applicable/No specific site mentioned
Special Codes
Special Code
No Value
CTCA Calls
Affordable Care Act (ACA)
In the news
Cancer Bulletin Ending
Recalcitrant Cancer Research Act
UCSF Study Call
Special Code 2 (same as 1)
Referrals Given
Referral 1
No Value
CIS information service
Smoking Quitline
Public Inquiries
POS
NCI Doc/Program
NCI Designated Cancer Center
NCI CCR/Clinical Center
NCCCP
CDC-BCCEDP
CDC-BCCEDP – Missouri
Genetics Services
Other Healthcare Facility
National or Community Org/Other Gov. Program
International Referral
Other
None
Break Off
Referral 2 (same as 1)
Referral 3 (same as 1)
Referral 4 (same as 1)
Referral 5 (same as 1)
Referral 6 (same as 1)
Follow-up Actions
Action 1
No Value
Sent information by mail
Emailed information
Social Media post
Warm transfer POS
Warm transfer org/agency
Scheduled call back
Other
Action 2 (same as 1)
Action 3 (same as 1)
Action 4 (same as 1)
Action 5 (same as 1)
Clinical Trials
Yes
No
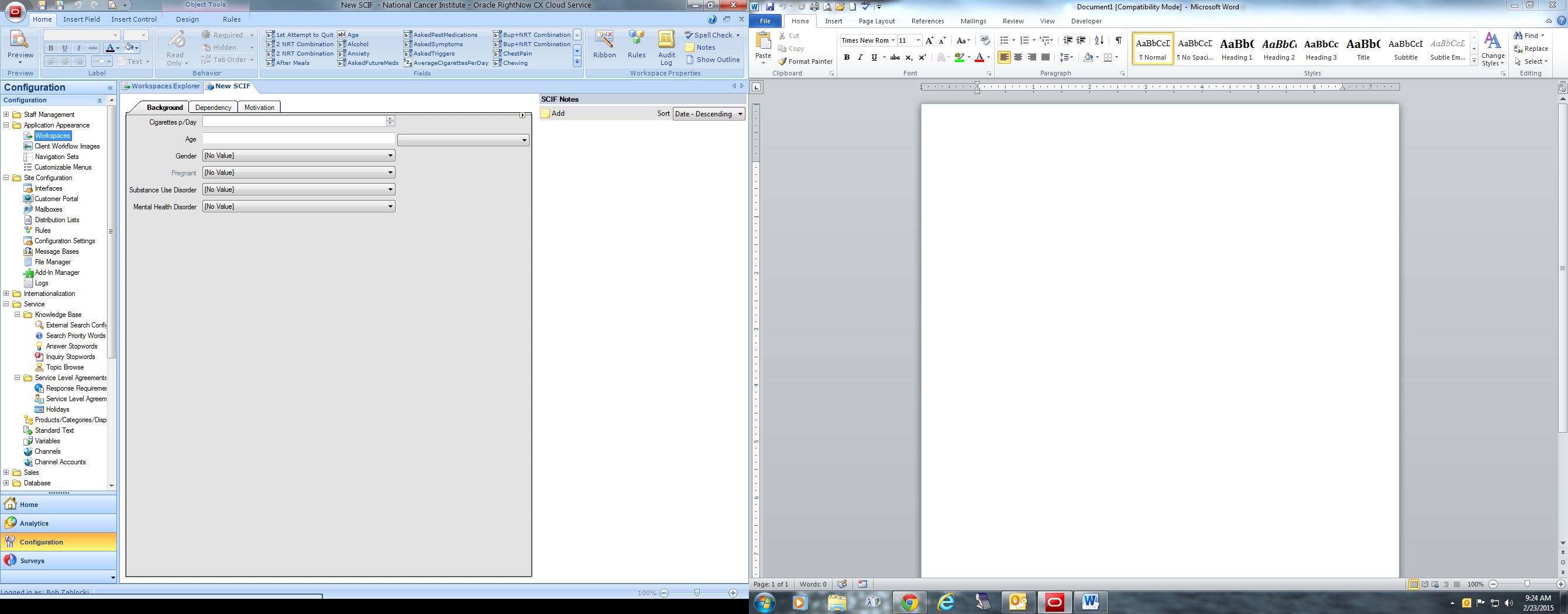
Background Screen
Cigarettes per Day
Age
Gender
Male
Female
Substance Use Disorder
Yes
No
Mental Health Disorder
Yes
No
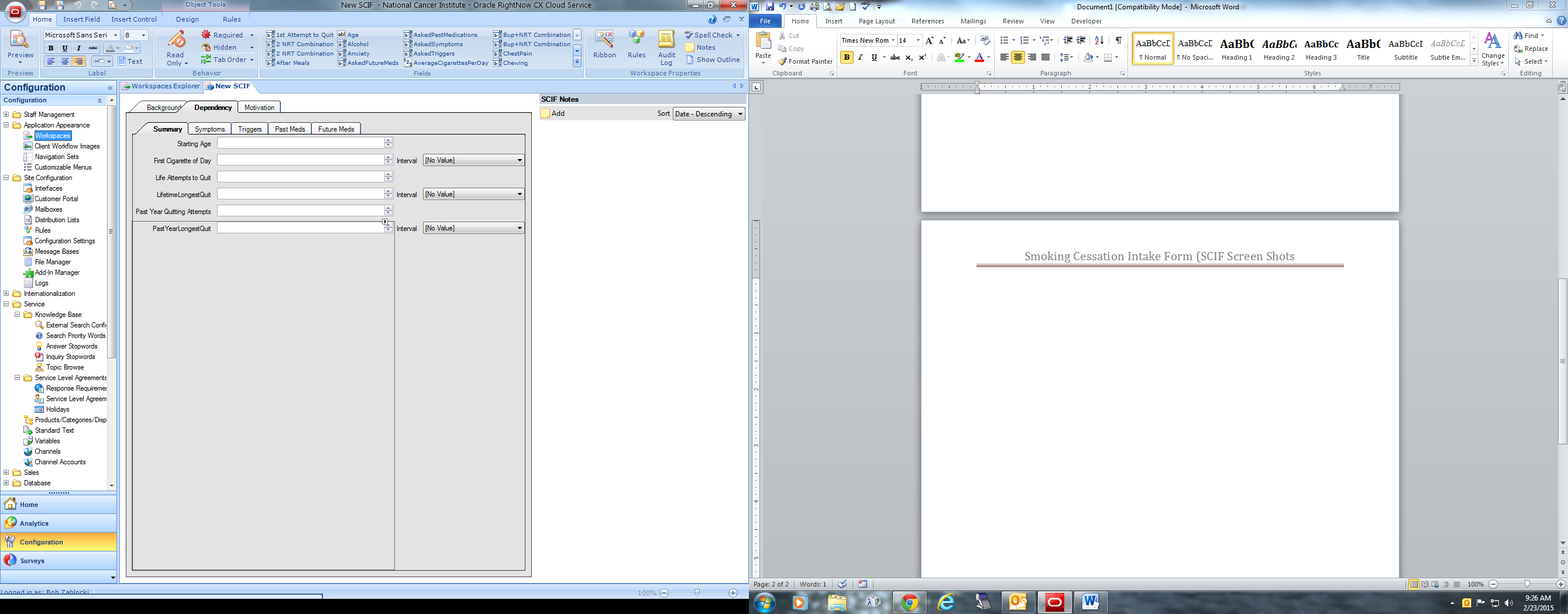
Dependency Screen:
Age when starting smoking cigarettes
First cigarette of the day after awakening
In life, number of quit attempts for 1 day or longer
Duration (beyond a day) of successful quitting
In past year, number of quit attempts
First call to the quit line in the past 12 months?
Longest time quit
Types of tobacco have you used in the past 30 days
Cigarettes
Menthol cigarettes?
Yes, I usually smoke menthol cigarettes
No, I usually smoke other types of cigarettes (non-menthol)
Don’t know
Refused
Not asked
Cigars, cigarillos, or little cigars
A pipe
Chewing tobacco, snuff, or dip
Any other type of tobacco
Last time smoked a cigarette, even a puff :
dd/mm/yyyy
Don’t know
Refused
Not asked
Avg. Number of cigarettes smoked each day ___
Currently smoke cigarettes every day, some days, or not at all? (Note: “currently” refers to right now, today.)
Everyday
Some days
Number of days smoked in the last 30 days: ___
Don’t know
Refused
Not asked
Not at all
Don’t know
Refused
Not asked
Age?
Sex?
If female, are you pregnant right now?
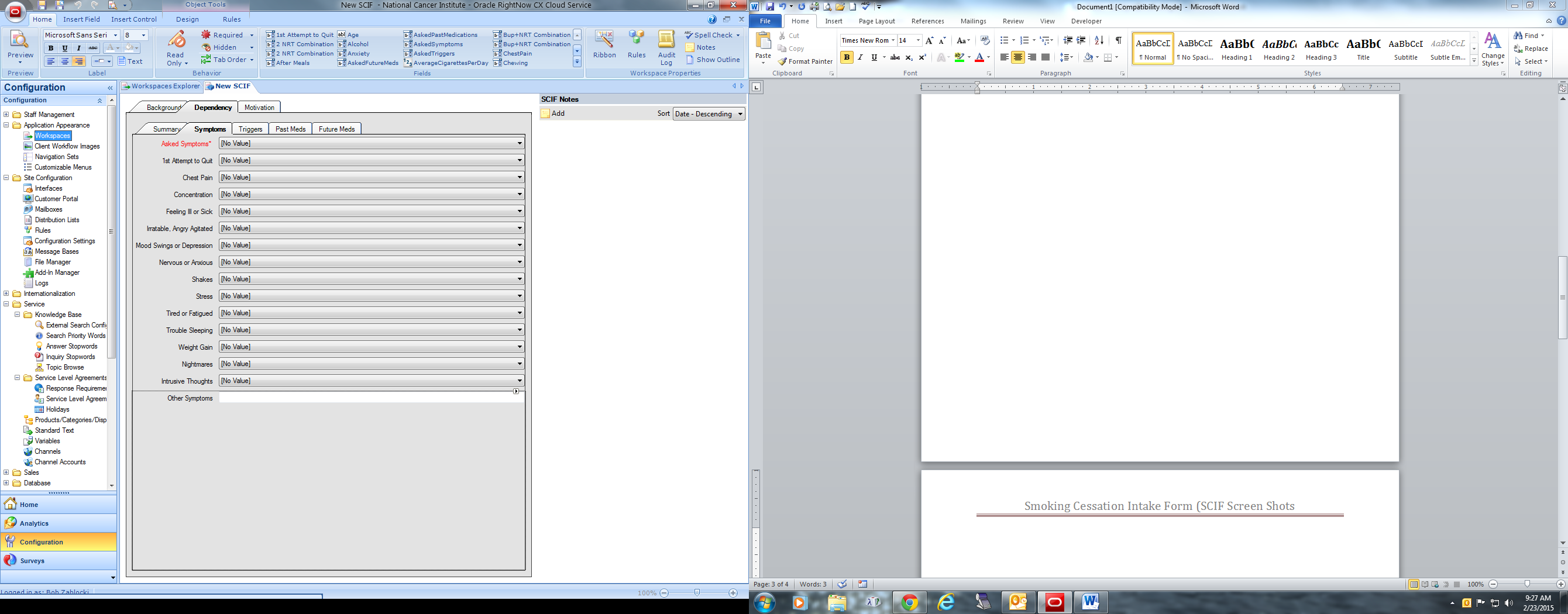
Symptoms experienced after quitting
Feeling irritable, angry, agitated
Mood swings, depressed, down, or blue
Nervous, anxious, jumpy
Cravings
Trouble sleeping, nightmares, dreams
Has not tried to quit before (1st quit attempt)
Weight gain
Increased appetite or hunger
Tired, fatigued
Feeling ill, sick, nausea, general malaise
Headache
Chest pain, shortness of breath
Stress
Unable to concentrate
Dizzy, lightheaded
Shakes
Other (please explain)
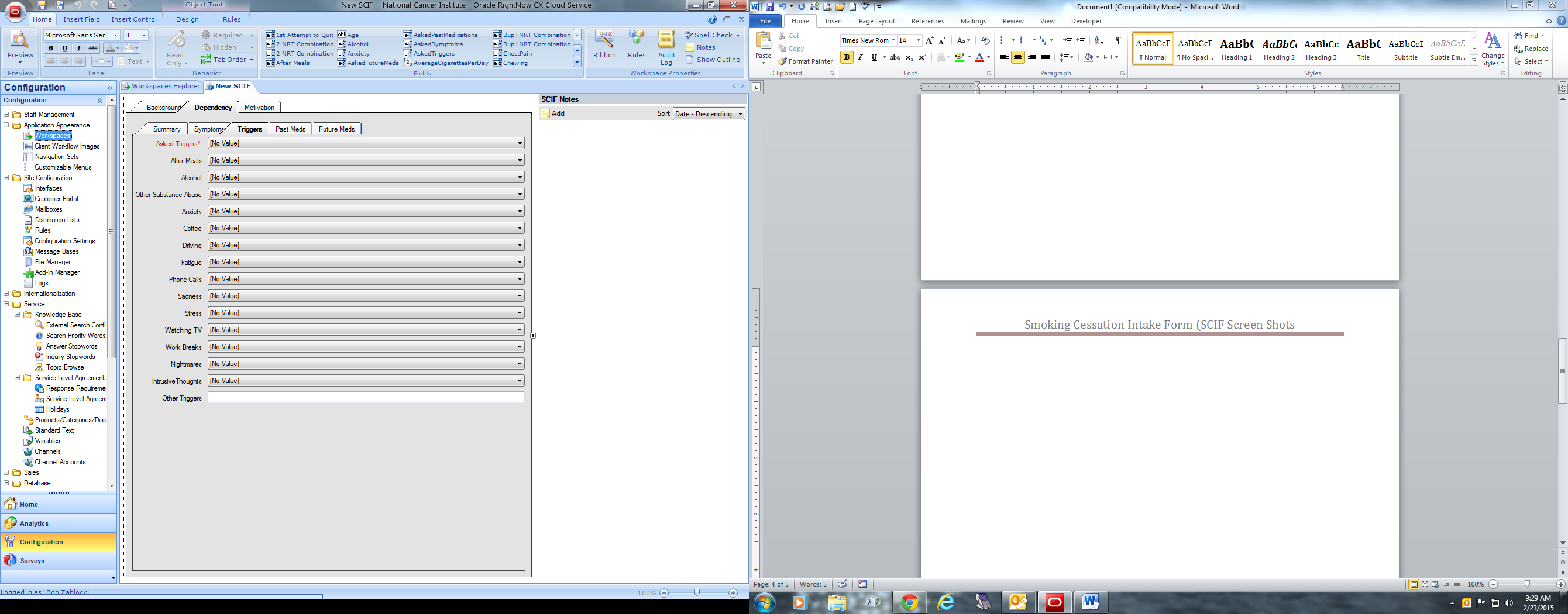
Triggers
Did not ask triggers
After meals
Alcohol
Other substance abuse
Anxiety
Coffee
Driving
Fatigue
Driving
Phone calls
Sadness
Stress
Watching TV
Work breaks
Nightmares
Intrusive thoughts
Other (please explain)
Past medication to quit
Did not ask
Used in past
Bupropion hydrochloride (e.g.Zyban, Wellbutrin)
Chantrix
Herbal
Inhalers
Lozenges
Nasal sprays
Patches
Policrilex gums
2 NRT combinations
Bup+NRT combination
Other
Future Meds
Did not ask
Not interested
Bupropion hydrochloride
Chantrix
Herbal
Inhalers
Lozenges
Nasal sprays
Patches
Policrilex gums
2 NRT combinations
Bup+NRT combination
Other
Comorbidity
Substance Abuse
Other
Motivation Screen Questions:
Most important reason for wanting to quit
Restrictions placed on smokers in restaurants, at work, and other public places
Family or friends
To feel more in control of your life
To improve your health
To save money
To improve your health
Because your doctor told you to
Because of your children (grandkids)
For a healthy pregnancy
Just tired of smoking
Professionalism, Role model
Religious reasons
Extracurricular activities (e.g. basketball, jogging, dancing, volleyball, etc.)
Age
Concern about cancer prompted by death of family member or public figure
Dirty/bad habit
Other (please explain)
Did not ask
Secondary Reason?
See examples from last question
No other reason
Did not ask
Others in the household currently using tobacco products (one or more)
Other Users?
Child?
Friend?
Parent?
Partner?
Household Tobacco Products Used
Chewing
Cigarettes
Cigars
Pipes
Snuff
Quitting
Quitting next 30 days?
Quit date
Confidence in Quitting
No value
Somewhat confident
Confident
Neutral
Not confident at all
Call Backs?
Interested in call back?
Agree to terms of service?
| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| File Title | Smoking Cessation Intake Form (SCIF Screen Shots |
| Subject | SMOKING CESSATION INTAKE FORM (SCIF) with SCREEN SHOTS |
| Author | Burstyn, Ilene (NIH/NCI) [E] |
| File Modified | 0000-00-00 |
| File Created | 2021-01-24 |
© 2026 OMB.report | Privacy Policy