Form 1 Understanding and Monitoring Funding Streams in Ryan Whi
Understanding and Monitoring Funding Streams in Ryan White Clinics
Attachment A - Survey Instrument_Draft_2014 Final Revisions
Understanding and Monitoring Funding Streams in Ryan White Clinics Survey
OMB: 0915-0377
Attachment A. Survey
OMB No. 0915-XXXX
Expiration date: XX/XX/201X
Understanding and Monitoring Funding Streams in Ryan White Clinics - Survey
|
Supported by the Health Resources and Services Administration, HIV/AIDS Bureau Contract Number: HHSH250200646016I |
Public Burden Statement: An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it displays a currently valid OMB control number. The OMB control number for this project is 0915-XXXX. Public reporting burden for this collection of information is estimated to average XX hours per response, including the time for reviewing instructions, searching existing data sources, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to HRSA Reports Clearance Officer, 5600 Fishers Lane, Room 10-29, Rockville, Maryland, 20857.
Message to Respondent
Thank you for participating in the study, Understanding and Monitoring Funding Streams in Ryan White Clinics. Your response to the survey is crucial in providing HAB and policymakers with a better understanding of how the RWHAP currently provides primary outpatient health care and essential support services to both uninsured and underinsured clients. It will identify what types of core medical services and subservices, and support services are currently not covered or not fully covered by Medicaid, Medicare, and private insurance, which are needed to provide high quality HIV/AIDS care. The study also will provide information on how grantees monitor patient healthcare coverage (e.g., payer source, type of insurance) and the cost of care. Together, this information will help HAB understand how Part C and Part D grantees support and track expanded health insurance enrollment for their clients and to adapt to the changing funding landscape.
The study will also collect information on what processes are used and what types of data are stored within grantee data information systems. Information about data information systems will be used to support the development of a technical assistance tracker for RWHAP grantees to monitor and assess changes in the mix of funding sources used to pay for primary health care and essential support services to PLWHA as the Patient Protection and Affordable Care Act is fully implemented.
The following survey is intended to capture as much information on your agency’s financial systems and tracking practices. You may find that some of the questions posed may not reflect your agency’s practices. In these instances, please use the comment boxes to provide a description of your agency’s actual practices. For some questions where “Other” is an option, again please provide an explanation in the space provided. The additional comments you provide are essential in informing the design, features, and capability of the technical assistance tracker.
We will also have grantee peer-to-peer assistance and technical assistance available to help you complete the survey. If you need assistance in answering the survey, please contact:
West
Coast: Tessa Robinette at (916) 239-4020 ext. 232 or
trobinette@wrma.com
East Coast: Imogen Fua at (301) 881-2590
ext. 272 or ifua@wrma.com
Thank you for your time and support.
GRANTEE DEMOGRAPHIC INFORMATION
Agency name _______________________________________________
Agency Location (city, state) ___________________________________
Respondent Name ____________________________________________
Respondent’s Title ___________________________________________
Respondent’s Telephone Number _______________________________
Respondent’s Email Address ___________________________________
Is your program/facility that provides services to persons living with HIV or AIDS (PLWHA) recognized as a Patient Centered Medical Home (PCMH) (also known as a Primary Care Medical Home)?
Yes
We are currently seeking recognition
No
7a. If yes, when were you recognized? ________________
If you have any additional comments, please provide them below:
As you know, the Centers for Medicare and Medicaid Services (CMS) is providing funding for States to establish health homes for people with Medicaid with 2 or more chronic conditions through the election of the Medicaid State plan option for establishing health homes. Is your program/facility participating in part of a state sponsored initiative for the establishment of health homes (as provided in the Patient Protection and Affordable Care Act)?
Yes, we are a designated provider
No, we are working with our Medicaid agency on electing the Medicaid State plan option to develop health homes for PLWHA
No, we are not working on establishing a health home
Not applicable in our state
If you have any additional comments, please provide them below:
How many full time equivalents (FTEs) does your agency employ as primary care providers serving PLWHA? ________
Please describe your agency’s relationship with private Managed Care Organizations (MCOs). [Check all that apply]
o Individual HIV clinicians participate in MCO network(s) as primary care providers (PCPs)
o Individual HIV clinicians participate in MCO network(s) as specialists
o HIV clinic participates in MCO network(s)
o The umbrella organization/hospital participates in MCO network(s)
No participation
Other (please describe), _______________________________________________
If you have any additional comments, please provide them below:
Please describe your agency’s relationship with Medicaid Managed Care Organizations (MCOs). [Check all that apply]
o Individual HIV clinicians participate in networks as primary care providers (PCPs)
o Individual HIV clinicians participate in networks as specialists
o HIV clinic participates in networks
o The umbrella organization/hospital participates in networks
o No participation
If you have any additional comments, please provide them below:
If your HIV clinicians are part of an MCO, how is your program reimbursed?
Fee for service
Capitated (per member per month)
N/A
If you have any additional comments, please provide them below:
Please check the services your agency provides to PLWHA directly or through contracts with other provider(s) [Check all that apply]
Outpatient ambulatory care
Oral health care
Mental health services
Medical nutrition therapy
Medical case management
Substance abuse services
HIV counseling and testing
Non-medical case management
Child care services
Pediatric development assessment/early intervention services
Emergency financial assistance
Food bank/home-delivered meals
Health education/risk reduction
Housing services
Legal services
Linguistic services
Medical transportation services
Outreach services
Permanency planning
Psychosocial support services
Referral for health care/support services
Rehabilitation services
Respite care
Substance abuse-residential
Treatment adherence counseling
Other _____________________________________________________
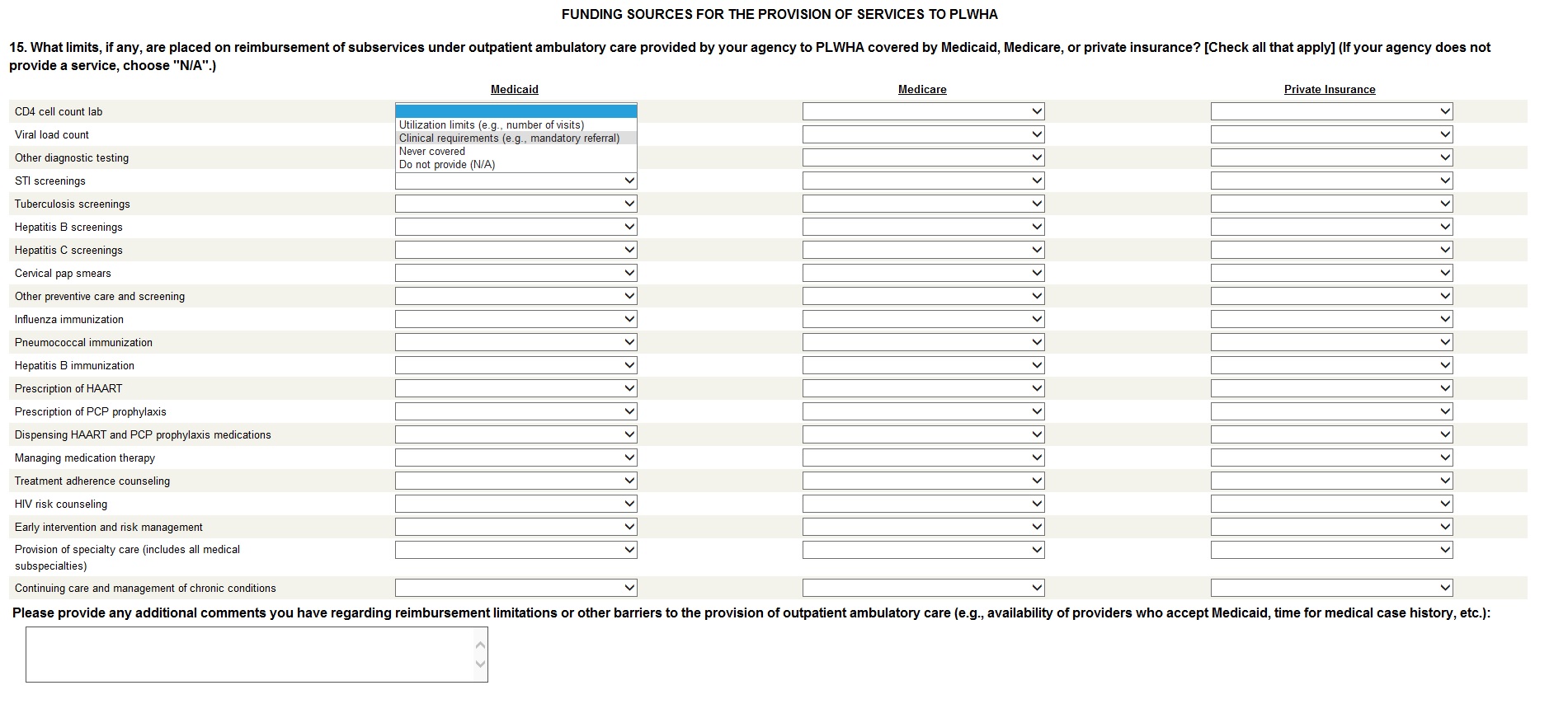
FUNDING SOURCES FOR THE PROVISION OF SERVICES TO PLWHA
Are there any limits placed on reimbursement of subservices under outpatient ambulatory care provided by your agency to PLWHA covered by Medicaid, Medicare or private insurance? If your agency does not provide a service, check "N/A." If there are limits placed on reimbursement, check the appropriate boxes.
Service reimbursement limitations: |
Do not Provide (N/A) |
Medicaid |
Medicare |
Private Insurance |
||||||
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
||
CD4 cell count lab |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Viral load count |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Other diagnostic testing |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
STI screenings
|
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Tuberculosis screenings |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Hepatitis B screenings |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Hepatitis C screenings |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Cervical pap smears |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Other preventive care and screening |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Influenza immunization
|
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Pneumococcal immunization |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Hepatitis B immunization |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Prescription of HAART |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Prescription of PCP prophylaxis |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Dispensing HAART & PCP prophylaxis medications |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Managing medication therapy |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Treatment adherence counseling |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
HIV risk counseling |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Early intervention and risk management |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Provision of specialty care (includes all medical subspecialties) |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Continuing care and management of chronic conditions |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Please provide any additional comments you have regarding reimbursement limitations or other barriers to the provision of outpatient
ambulatory care (e.g., availability of providers who accept Medicaid, time for medical case history, etc.). Also provide any comments if you cannot answer any or all of Question 14:
Are there any limits placed on reimbursement of additional medical and support services provided by your agency to PLWHA who are covered by Medicaid, Medicare or private insurance? If your agency does not provide a service, check "N/A." If there are limits placed on reimbursement for additional medical or support services, check the appropriate boxes.
Service reimbursement limitations: |
Do not Provide (N/A) |
Medicaid |
Medicare |
Private Insurance |
||||||
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
Utilization limits (e.g., number of visits) |
Clinical requirements (e.g., mandatory referral) |
Never covered |
||
Oral health care |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Mental health services |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Medical nutrition therapy |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Medical case management |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Substance abuse services |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
HIV counseling and testing |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Non-medical case management |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Health education/risk reduction |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Medical Transportation services |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Rehabilitation services |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Substance abuse – residential |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
☐ |
Please provide any additional comments you have regarding reimbursement limitations or other barriers to the provision of the medical and support services listed above. Also provide any comments if you cannot answer any or all of Question 15:
INFORMATION ON GRANTEES’ ABILITY TO TRACK HEALTH INSURANCE AND FUNDING SOURCES |
Tracking of Insurance Status |
|
|
|
|
Do you have/receive information regarding reimbursements received from Medicaid or private health insurance for PLWHA clients you serve?
Yes, the Ryan White program at my agency can easily access this information
Yes, but the information is difficult to access
No
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ryan White Technical Assistance (TA) Service Tracker Tool
HAB is developing a Ryan White Technical Assistance (TA) Service Tracker for Ryan White grantees that will allow Part C and D grantees to better understand the interrelationships of funding streams used to support comprehensive HIV/AIDS care and to document the role of the Ryan White Program in ensuring that PLWHA receive high quality care. The tracker will consist of an Access database, into which grantees can import data in a standardized format on a routine basis. The tracker will be for grantees themselves. It will not involve any additional data reporting to HAB. To help understand the feasibility of including cost or reimbursement information in the tracker, we would like to ask you some questions about whether and how you capture financial information.
Ability to Estimate Cost of HIV/AIDS Care by Funding Source and Service Category
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
22a. If yes, what is the most recent estimate for the average annual cost of services provided and/or contracted by your agency for PLWHA? __________________
22b. If yes, please explain your methodology for calculating the cost of care.
For example, if your agency wanted to calculate the total revenue from the provision of oral health care to PLWHA in 2012, would you be able to understand how much of this figure comes from Medicare reimbursement, how much from Ryan White, how much from private insurance, etc.?
23a. If “Yes, easily,” please describe your process. This may include your process for identifying a client’s health insurance status and the services covered by that insurance (Skip to 25).
2
Potential Use of the Ryan White Services Tracker
The tracker will produce a series of tables and graphs summarizing services over time (and funding sources if available). Please fill out the below questions below to help with the design of the tracker.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
25a. If “Yes” or “No, but most data are captured in one system.” What is the system?
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
25b. At what level do you capture services in this system? [Check all that apply]
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
25c. Do you assign insurance/reimbursement source/payor source to services in this system?
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
SPECIFIC DATA ON FUNDING SOURCES USED TO PROVIDE SERVICES
FOR PLWHA
Healthcare providers may maintain and report different records according to different calendars. For example, fiscal information may be maintained along a July-June calendar while service information may be maintained along a January-December calendar.
For the questions below, please provide your answers according to the most appropriate calendar corresponding to the 2012 year. This may mean the service information you provide corresponds to a different 2012 calendar than funding or grant information.
In 2012, how many PLWHA did your agency serve (including non-Ryan White clients)? ________________________________
How much revenue did you receive (in dollars) from each Part of the Ryan White HIV/AIDS Program in 2012? (Please indicate 0 if none was received)
Part A: _____________________________
Part B: _____________________________
Part C: _____________________________
Part D: _____________________________
Part F: _____________________________
How much reimbursement did you receive (in dollars) from Medicaid, Medicare, and/or private insurance for the provision of services to PLWHA in 2012? (Please indicate 0 if none was received and indicate N/A if unknown or unable to estimate.)
Medicaid: _____________________________
Medicare: _____________________________
Private Insurance: _______________________
How much revenue (if any) did you receive for HIV/AIDS-related services from other sources in 2012? If none, please indicate zero.
All Other Funding Sources: ______________________
Did you use any of your Ryan White Part C and/or Part D funds for salaries (FTEs) in 2012?
Yes (Please answer 32a)
No (end)
31a. If yes, how many FTEs? ________
31b. How much of your Part C and/or Part D funds (in dollars) do these salaried FTEs represent?
Part C: ________
Part D: ________
31c. Please check the services provided by these FTEs. [Check all that apply]
Outpatient ambulatory care
Oral health care
Mental health services
Medical nutrition therapy
Medical case management
Substance abuse services
Non-medical case management
Child care services
Pediatric development assessment/early intervention services
Emergency financial assistance
Food bank/home-delivered meals
Health education/risk reduction
Housing services
Legal services
Linguistic services
Medical transportation services
Outreach services
Permanency planning
Psychosocial support services
Referral for health care/support services
Rehabilitation services
Respite care
Substance abuse-residential
Treatment adherence counseling
HIV counseling and testing to determine the presence of HIV infection
Other (Please specify): ___________________________________________________
Screen Shots of Survey Instrument


| File Type | application/vnd.openxmlformats-officedocument.wordprocessingml.document |
| Subject | Understanding and Monitoring Funding Streams in Ryan White Clinics VERSION 2 |
| Author | loppenheim |
| File Modified | 0000-00-00 |
| File Created | 2021-01-28 |
© 2026 OMB.report | Privacy Policy